Covid 1/7: The Fire of a Thousand Suns
post by Zvi · 2021-01-07T17:00:01.843Z · LW · GW · 56 commentsContents
The Numbers
Predictions
Deaths
Positive Test Percentages
Positive Tests
Test Counts
Covid Machine Learning Project
Vaccinations
Europe
The English Strain: Are We F***ed? Is it Over?
The South African Strain: Are We Even More Fucked? Is It Even More Over?
But What Do We Do Now?
What Should You Do Personally?
It is worth securing your supplies in case the supply chain becomes an issue. The earlier you do that, the more measured you can be doing it, and the better it is for everyone.
Unless you are immune, at some point, whether or not you decide that point is already here, there is a high chance you will want to start taking extreme precautions. Be ready. If you have to choose, better to take your necessary risks now, rather than later.
Two Dose, One Dose, Who Knows, You Knows
Yes, We Can Agree Andrew Cuomo Is The Worst
All I Want For Christmas is a Covid Vaccine, But They Somehow Underpriced Them So Much No One’s Even Bothering To Sell Out
The conclusion is clear as day. If we cared about distribution of the vaccine, the vaccine would be distributed. Period.
Vaccine Allocation By Politics and Power
How Bad is it Out There Right Now?
In Other News
None
56 comments
I’ll summarize everything up front.
Might as well get on with it.
Let’s do the numbers.
The Numbers
Predictions
Prediction last week: 14.3% positive rate on 9.7 million tests, and an average of 2,500 deaths, again with wide error bars.
Results: 16.4% positive rate on 9.3 million tests, and an average of 2,657 deaths.
The phase shift on 12/30, in the wake of Christmas, seems to have been real, giving us the clear holiday bump we did not see from previous holidays.
That was both the very bad outcome for infections I was worried about, and also not high on my list of things to be concerned or furious about this week.
For deaths, my estimate was lower than it should have been and I should have assumed a full reversion, so on reflection it’s my mistake rather than especially bad news.
The new strain is not yet prevalent enough to be noticeably impacting the numbers.
Prediction: 17.0% positive rate on 9.5 million tests, and an average of 2,800 deaths. The holidays are over, there will be some fallout, with things getting slightly worse, but with the main boost in deaths from Christmas mostly coming later.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Oct 29-Nov 4 | 956 | 1977 | 2309 | 613 |
| Nov 5-Nov 11 | 1089 | 2712 | 2535 | 870 |
| Nov 12-Nov 18 | 1255 | 2934 | 2818 | 1127 |
| Nov 19-Nov 25 | 1761 | 4169 | 3396 | 1714 |
| Nov 26-Dec 2 | 1628 | 3814 | 2742 | 1939 |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
| Dec 10-Dec 16 | 3278 | 5324 | 4376 | 3541 |
| Dec 17-Dec 23 | 3826 | 5158 | 5131 | 3772 |
| Dec 24-Dec 30 | 3363 | 3668 | 4171 | 3640 |
| Dec 31-Jan 6 | 5320 | 5036 | 6072 | 4986 |
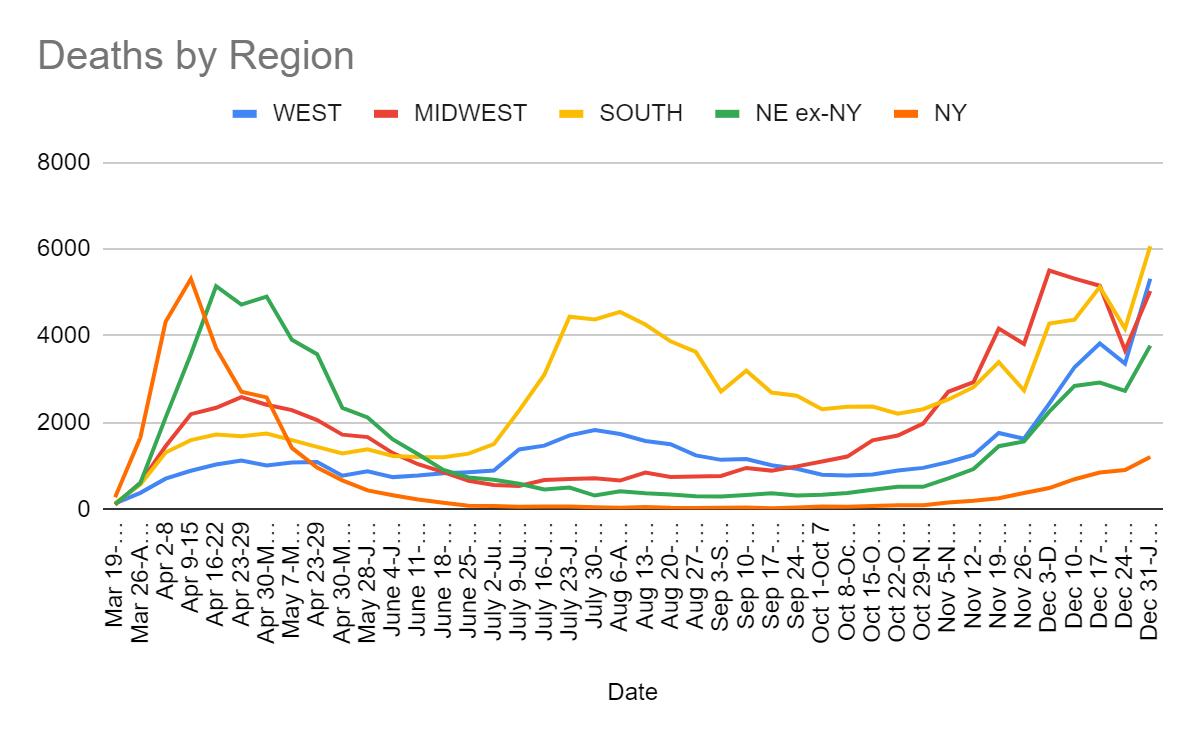
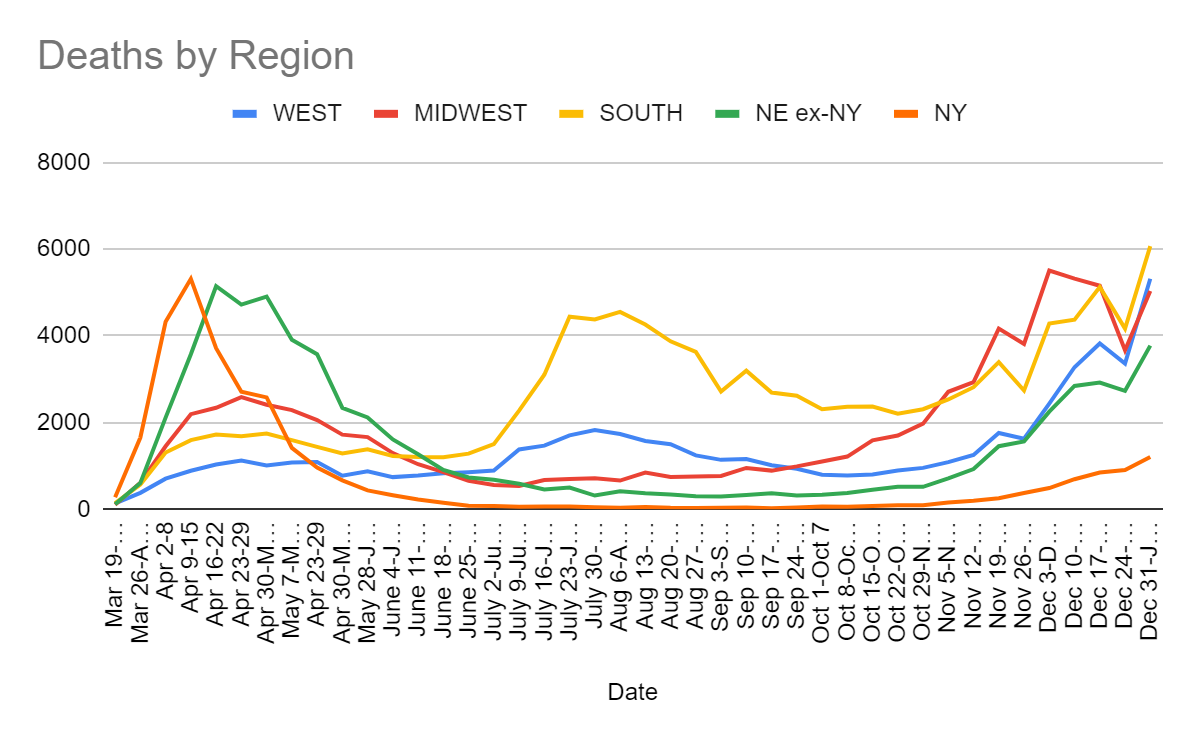
This is the one place it’s not as bad as it looks. The data source for these numbers is Wikipedia, which shows a relatively large amount of shifting of deaths from last week into this week.
If we assume that a lot of this week’s deaths were actually last week, that explains much of the increase. It’s not good news or anything, it’s definitely bad news, but it is not full on terrifying like it would be if we didn’t know about Christmas.
We still should expect further increases in the next few weeks before the tide likely temporarily turns.
Positive Test Percentages
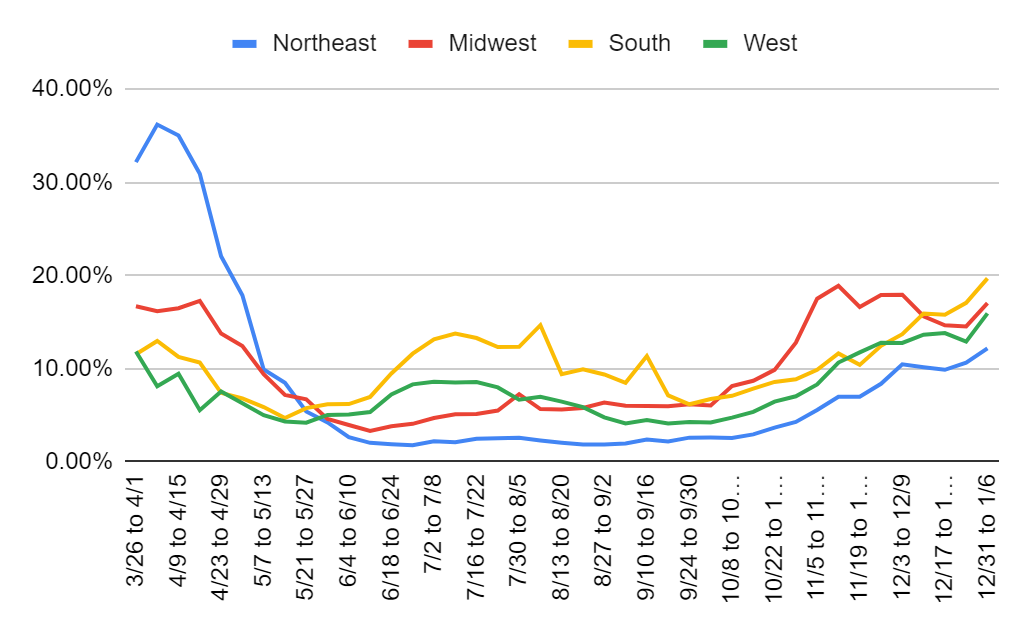
| Percentages | Northeast | Midwest | South | West |
| 11/5 to 11/11 | 5.56% | 17.51% | 9.89% | 8.31% |
| 11/12 to 11/18 | 6.99% | 18.90% | 11.64% | 10.66% |
| 11/19 to 11/25 | 7.00% | 16.62% | 10.41% | 11.75% |
| 11/26 to 12/2 | 8.38% | 17.90% | 12.45% | 12.79% |
| 12/3 to 12/9 | 10.47% | 17.94% | 13.70% | 12.76% |
| 12/10 to 12/16 | 10.15% | 15.63% | 15.91% | 13.65% |
| 12/17 to 12/23 | 9.88% | 14.65% | 15.78% | 13.82% |
| 12/24 to 12/30 | 10.65% | 14.54% | 17.07% | 12.90% |
| 12/31 to 1/6 | 12.18% | 17.03% | 19.69% | 15.94% |
No way to sugar coat this one. Everything is pointed in the wrong direction in a clear phase shift. The good news is that it could be a one-time move from Christmas, and thus we can still plausibly expect things to remain stable from this point forward without waiting for further control systems to kick in. I hope to start seeing slow improvements soon, but I must admit that the overall graph is not as encouraging of that as I thought a few weeks ago, especially outside of the Midwest, and the turning point may be farther off than we’d like. The Midwest is still probably past its peak for this wave, even if everyone else has to wait a bit.
Positive Tests
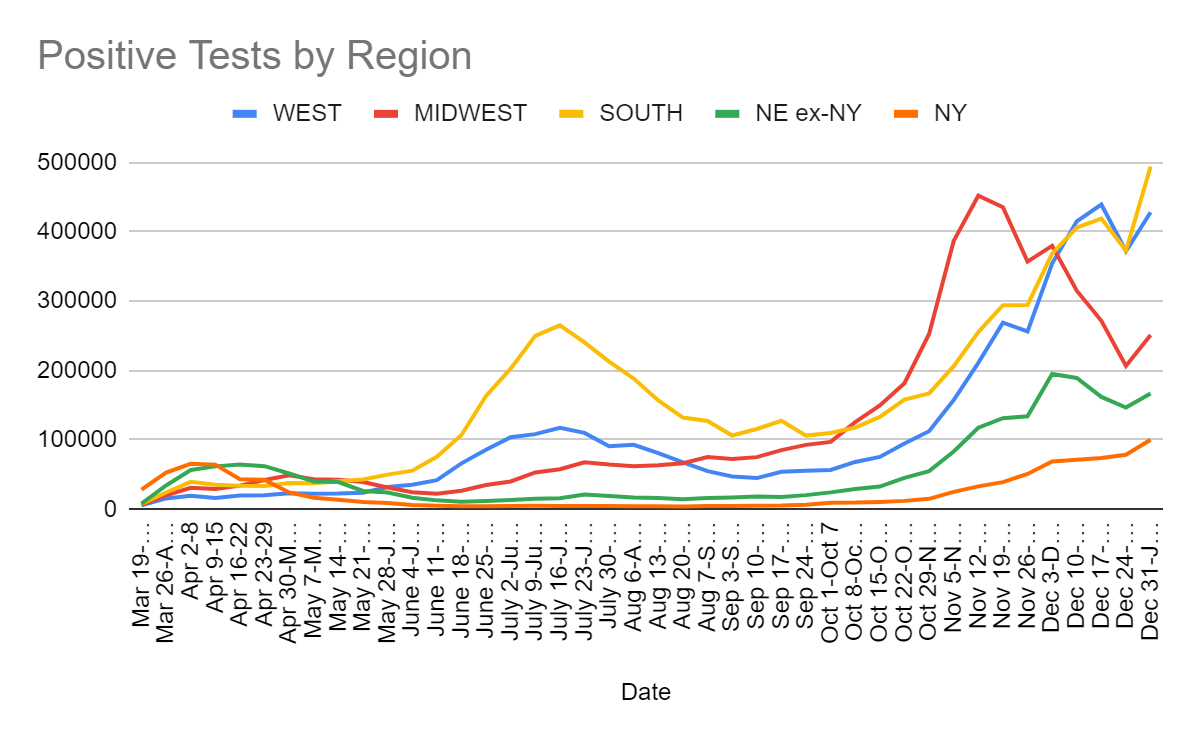
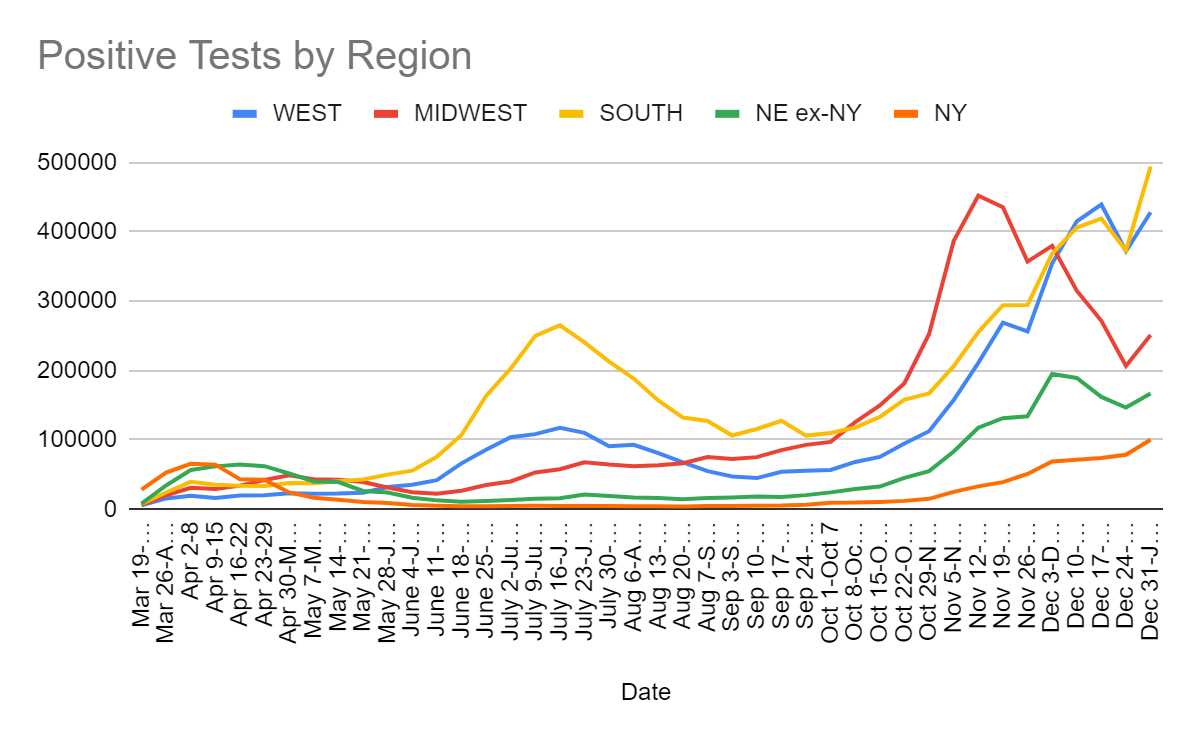
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Nov 12-Nov 18 | 211,222 | 452,265 | 255,637 | 150,724 |
| Nov 19-Nov 25 | 269,230 | 435,688 | 294,230 | 170,595 |
| Nov 26-Dec 2 | 256,629 | 357,102 | 294,734 | 185,087 |
| Dec 3-Dec 9 | 354,397 | 379,823 | 368,596 | 263,886 |
| Dec 10-Dec 16 | 415,220 | 315,304 | 406,353 | 260,863 |
| Dec 17-Dec 23 | 439,493 | 271,825 | 419,230 | 236,264 |
| Dec 24-Dec 30 | 372,095 | 206,671 | 373,086 | 225,476 |
| Dec 31-Jan 6 | 428,407 | 251,443 | 494,090 | 267,350 |
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Nov 5-Nov 11 | 8,290,417 | 10.8% | 1,059,559 | 2.4% | 3.16% |
| Nov 12-Nov 18 | 9,040,426 | 12.4% | 1,155,670 | 2.9% | 3.50% |
| Nov 19-Nov 25 | 10,419,059 | 11.8% | 1,373,751 | 2.9% | 3.88% |
| Nov 26-Dec 2 | 9,747,026 | 11.8% | 1,287,010 | 4.0% | 4.23% |
| Dec 3-Dec 9 | 10,465,254 | 13.9% | 1,411,142 | 4.9% | 4.67% |
| Dec 10-Dec 16 | 10,701,134 | 13.9% | 1,444,725 | 4.9% | 5.12% |
| Dec 17-Dec 23 | 10,716,189 | 13.7% | 1,440,770 | 5.1% | 5.57% |
| Dec 24-Dec 30 | 9,082,257 | 13.9% | 1,303,286 | 6.0% | 5.95% |
| Dec 31-Jan 6 | 9,317,985 | 16.4% | 1,365,473 | 7.3% | 6.42% |
The failure of test counts to recover here is maddening. We need to be adding more capacity, not taking multiple weeks off. The positive test percentages speak for themselves.
Covid Machine Learning Project
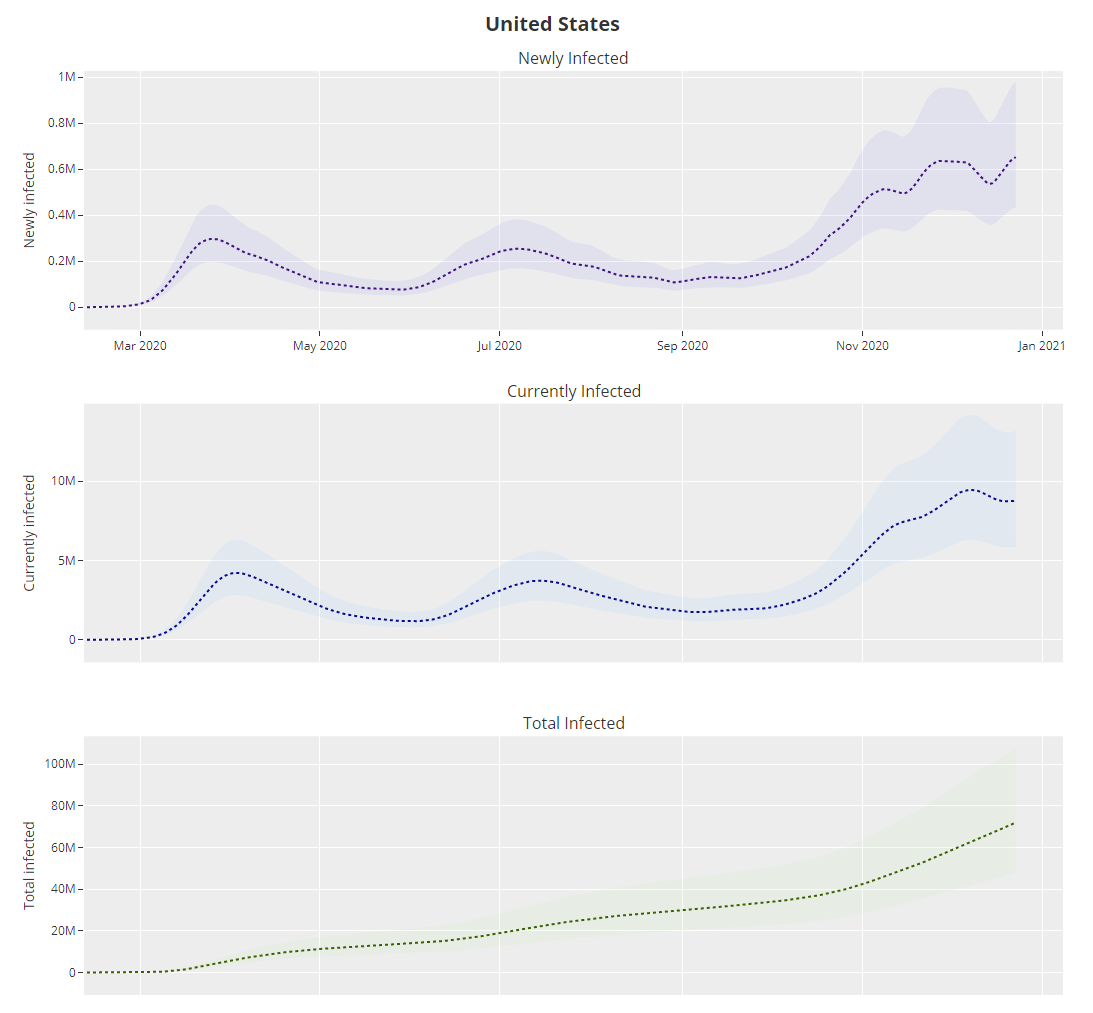
The code doesn’t know about Thanksgiving so it has a dip in infections in late November that clearly is not real, and now it is back to thinking R0 is over 1.1. Meanwhile, it had total infections on December 23 at 21.7%, versus a belief of 20.3% on December 16 last week, which it now thinks was 20.4% back then. Last week’s belief that things were steadily improving has been fixed by additional data to smooth out Thanksgiving.
Vaccinations
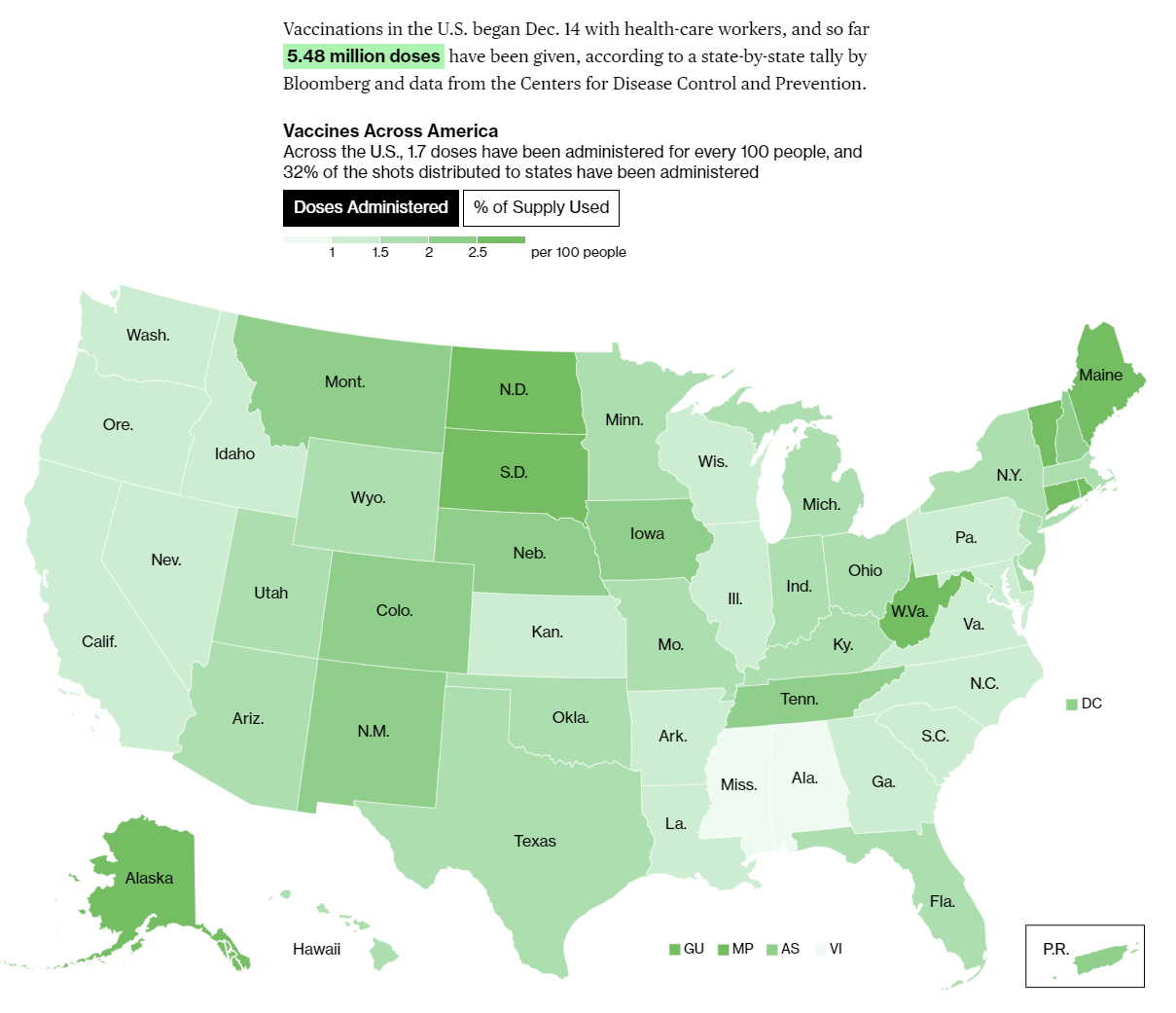
5.48 million doses so far, after almost a month. Pathetic. Scandalous. Insane. Shots. In. Arms. Now.
Europe
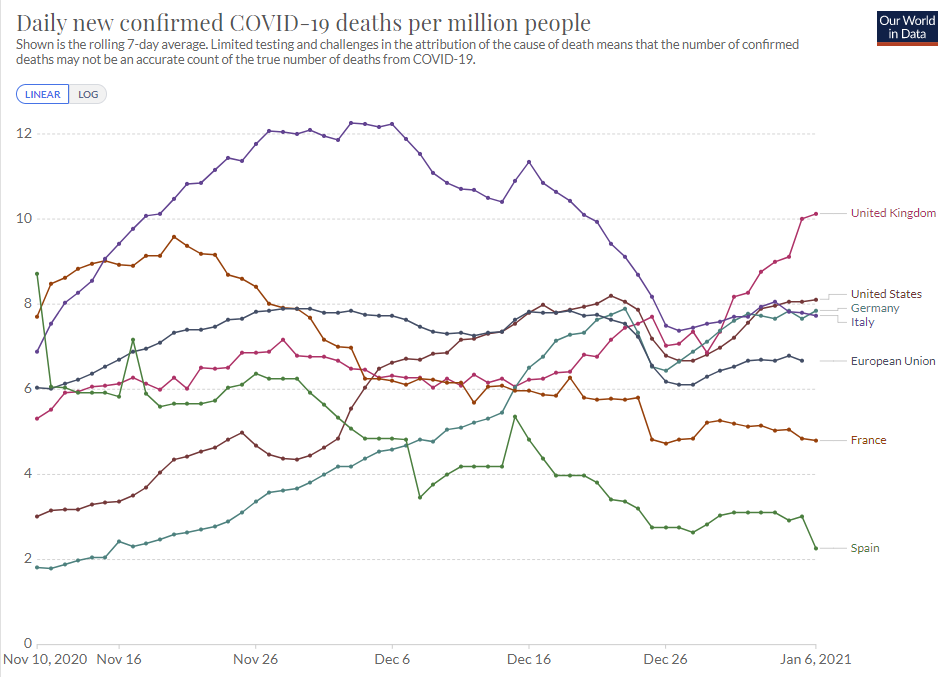
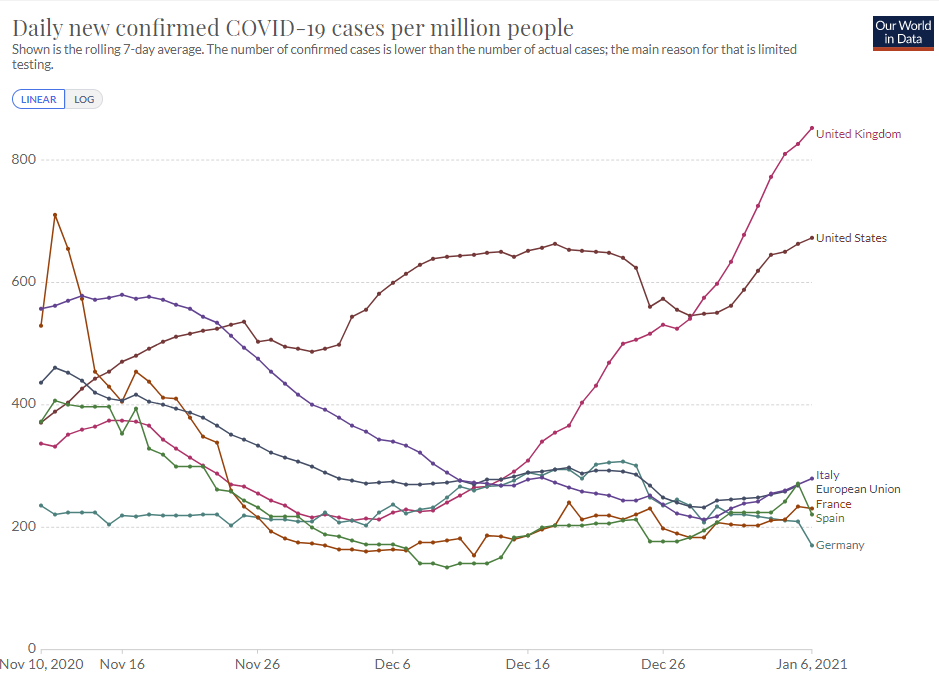
One of these lines is not like the others. The control system in the United Kingdom is failing.
The English Strain: Are We F***ed? Is it Over?
I found this comment very helpful, so I’ll quote it in full, it’s the best way I know of to estimate exactly how far along we are:
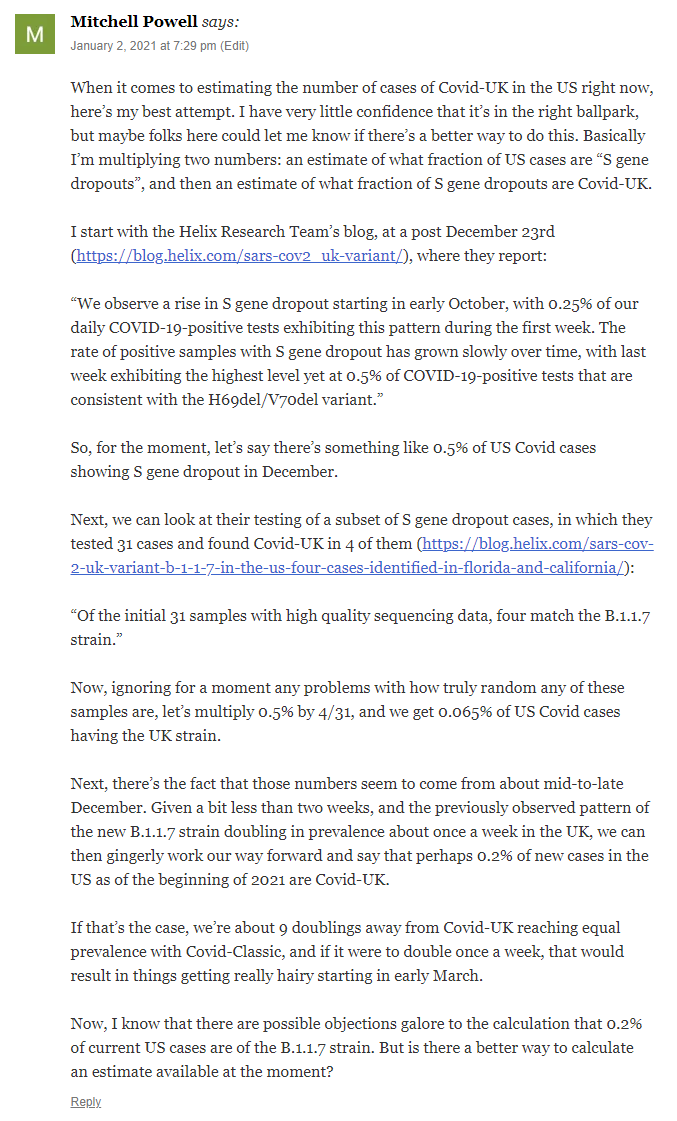
This is not a comforting picture. In my very quick and dirty first highly abstract model, with 50% more infectiousness in the new strain than the old, this would have us be 0.22% of the newstrain during the year’s first cycle, 2% by the end of January, 16% by the end of February, 68% by the end of March. In the simplest possible model that you should not in any way take seriously, the end of May would be the peak at roughly 225% of the infections per day we have now, July 1 we’d be back to where we are now, then a very rapid decline after that.
What evidence do we have about the infectiousness of the new strain?
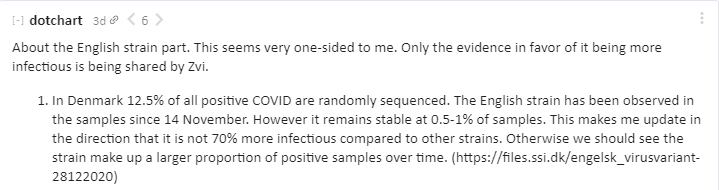
Denmark sequences the new strain, as a reason not to worry, a play in three acts:
Act One [LW(p) · GW(p)] (posted 12/31):
Asking “What evidence [LW · GW] filtered evidence? [LW · GW]” in situations like the new strain is important. I do my best to include all the evidence that’s worth including, but the degree to which I look for it might vary, and I could plausibly be doing things like not mentioning places where there is an absence of evidence that constitutes at least some evidence of absence. Please do keep calling me out on such mistakes by pointing out what’s missing, with or without the principle of charity.
Act Two [LW(p) · GW(p)] (posted 12/31 in reply):

(I hadn’t posted the Denmark data last week because I hadn’t seen anything that led me to update substantially in either direction, sample sizes and magnitudes seemed too low.)

So that looks… exactly like what you would see with a 65% more infectious strain, which doubles about once per week, while other evidence points me closer to about 50% more infectious than 65%. I’m essentially assuming at this point that the new strain is at least substantially (35%+) more infectious.
I don’t know what the likelihood ratio on this was, but it seems pretty damn high. And that’s the one country I had heard was doing a bunch of sequencing other than the United Kingdom, on one of only two strains we are worried about. So it seems not very selected. But I could easily be missing awareness of others, if so please do share.
Did I mention most European schools are still open? Well, here’s some news:
The San Diego case of the new strain gets contact traced, the results are in and 32 more cases have been found:
If he’s right about the current prevalence being ~1%, that’s not comforting. Quite the opposite. That’s two weeks ahead of my previous estimated schedule, and the one I used for the spreadsheet modeling. Which gives us two less weeks to vaccinate, and for temperatures to improve, before we get hit hard. The good news is that the naive model doesn’t think this does that much additional damage, mostly moving infections forward in time, although it does make the last peak a little bigger and the total infection count a little higher.
In other evidence (source 1, source 2):




At this point, if this were outside the range of 40%-75% more infectious, I would be very surprised.
The South African Strain: Are We Even More Fucked? Is It Even More Over?
Don’t look now, actually do look, we might actually truly be Malcom Reynolds “It’s worse than you think” level fucked by the South African strain, in which case it might be really, really over:
Here’s another source that seems to be further along in its analysis, linked paper here:
This is the kind of thing you see all the time from such sources, and such sources are capable of being a lot louder than this on such things even on very false alarms, so I don’t put too much weight on them yet.
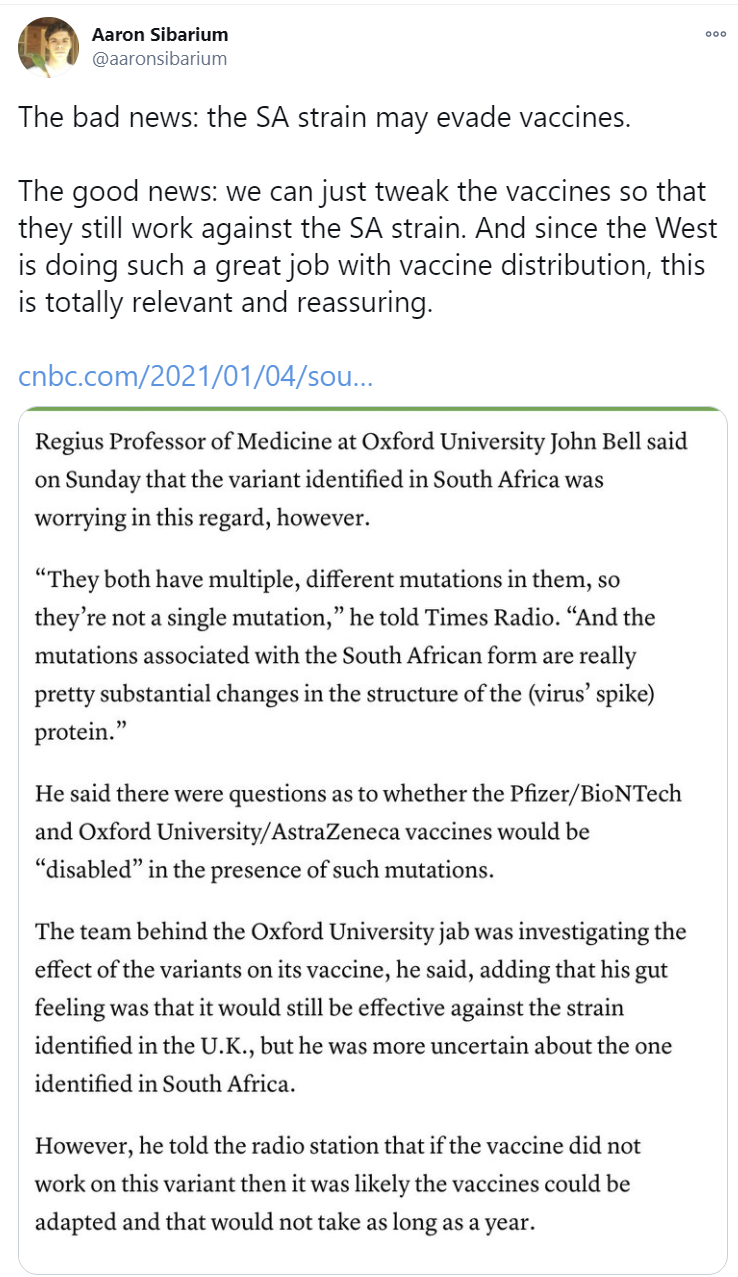
The problem is, I asked my father, who taught immunology at Columbia University and had a business doing due diligence on pharmaceutical companies, to look into the situation, and what he told me was very much not encouraging.
Here is what he came back with:
“A variant isolate of SARS-CoV2 from South Africa is causing concern, because convalescent sera from some patients recovered from infection with the predominant strain, while effective in neutralizing the same strain, were not effective in neutralizing the South African variant. Sera from other such patients did neutralize the variant effectively.
The concern is whether the current mRNA vaccines (coding for the spike protein from the predominant strain) will be effective against the variant. Unfortunately, the authors did not test sera from vaccinated individuals against the variant, so we don’t know for sure. It may be widely effective, effective in some individuals but not in others, or widely ineffective in provoking synthesis of neutralizing antibody to the variant.
A wrinkle: The current vaccines may offer protection from serious illness even in individuals in whom it fails to provide neutralizing antibody, but unlikely to prevent infection.
One of the advantages of the mRNA vaccines is that their manufacture can be modified quickly to accommodate changes. One would hope that the new vaccines could be granted emergency approval quickly, since they would be very similar to the approved ones.”
In conversation, he put the probability that the new variant would interfere with the neutralizing agent of the antibodies generated by those who get the mRNA vaccines at 80%. This is something we can find out quickly through experimentation, and it’s a sign of how bad we are at running experiments that the news has not yet (to my knowledge) reached us. There’s also the chance that other forms of protection could help out, or that the neutralizing agent could still have substantial effects sufficient to prevent illness or reduce severity. But if it comes back that the worst case scenario is indeed the case, and this mutation allows mRNA-vaccinated people to become sick, and the strain is indeed otherwise more infectious than the old one, then we have a very big problem.
So the good news is that mRNA vaccines can quickly be modified to handle the new strain. And if we had a benevolent well-functioning government, we could recognize that it is the same vaccine still, and not require a new round of trials. I have very little hope that we would do this, and thus very little hope we would be able to make the necessary adjustments in a timely manner. I imagine the FDA and company holding up approvals of the new versions for several months, and then the exact same botched roll-out to happen again, and by then for it to be very much too late, even if we don’t face the mutation problem again.
The other good news is that it seems highly unlikely the new strain can do much reinfection of previously infected individuals, and that even if the trend of noticing more ‘reinfections’ is real, it isn’t going to move the bottom lines much. And also that it is possible we get actively lucky with all this, and the folks who are vaccinated can get infected but don’t get sick, which results in them having much more robust protection against future infection or more mutations than they got from the vaccine alone.
Anyone who knows more about this, please do chime in.
Now that we know we are fucked, and for the moment assuming for purposes of analysis that we’re not that fucked, the question then shifts to: Is it over?
But What Do We Do Now?
The same thing we do every night, Pinky. Tell everyone to Be Afraid. Be Very Afraid.
(That first part about vaccinations (MR) is completely right, of course.)
This “be more scared” is both people’s natural message to others, and also people’s natural reaction for themselves, for overlapping but also different reasons. When shown evidence that it’s going to get worse later, people ramp up their internal “this is bad” meter, and act more scared now. I know of one non-rationalist person who was shown my post on the new strain, and decided on the spot to head home, and that they were going to start staying home now and not see friends anymore.
I keep pointing out that on a personal level, in terms of your personal incentives, this is wrong.
If things are going to get much worse later, including a possible hospital system collapse, the new strain makes protecting yourself now less valuable to you, not more valuable. It’s now going to cost you much more to stay safe the whole way, and action later is going to be more risky than action now rather than less risky. So if you have risks you need to take to stay sane and/or stay solvent, or things that need attention like other medical concerns, better to take care of that now rather than later.
If you are thinking on a society-wide level, it’s complicated. Slowing spread also slows B.1.1.1.7, giving us a little more time to vaccinate before we need to fall back on our control systems. We might not entirely waste that time. It also means that when the control systems start to notice the new strain (which will happen at the same time regardless, because as I understand the math the strain takes over equally quickly regardless) it will be from a lower baseline level, so depending on exactly how the control systems function, we could get substantially better outcomes when the crisis hits.
On the other hand, you’re burning your remaining ammunition in terms of getting people to listen, lock down and play it safe. You’re also doing so in time for control systems to undo a lot of your work before the crisis hits. And if the hospitals are going to be overwhelmed in the future, to a much worse degree than they are now, then extra infections now could plausibly make the peak less bad, and thus reduce both deaths and the amount of overshoot.
None of which are questions anyone involved is thinking about. It’s one knob. Danger rising, sound alarms for danger, get people more scared, hope they act safer.
What Should You Do Personally?
What should you actually do on a personal level? I have been trying to get a better handle on that. I have a post from yesterday with some toy modeling attempts. It’s not my strong suit and it’s not going to be right, but so far I’ve seen essentially nothing, so giving it a go should hopefully inspire something better to follow.
What is clear is that there is a big difference between 50% and 65% more infectious. If we are looking at only 50%, the new strain will have a big impact, but if we can do a reasonable job (relative to current expectations, mind you) with vaccinations I’m growing more hopeful the final stage may not be too bad, and a range of outcomes seem plausible. If it’s 65%, I don’t see a way out of at least a brief period with a lot more infections than now, and our hope for keeping deaths down and hospitals intact is based on getting enough of the vulnerable vaccinated by then.
Therefore, keep a close eye on which scenario we are looking at, and how things are playing out otherwise. It really does change what behaviors make sense.
If the cost of protecting yourself for long enough is high, that makes the value of staying safe now lower. Getting infected now is not good, the hospitals are already not in a great place, but things could get much worse.
I won’t go over in detail what ‘stay safe’ means, but it means all the things you’d think: Socially distance, wear masks, take Vitamin D, do things and meet people outdoors, check for symptoms, check air ventilation. I continue to think surfaces are a trivial worry beyond washing one’s hands, although if one is trying to be actively super paranoid (e.g. in a hospital collapse) precautionary principle is reasonable.
As a reminder, death rates from Covid-19 for young healthy people are quite low, but there are potential long-term consequences and medium-term consequences that we have large uncertainty about with regard to both frequency and magnitude (because experimentation and data gathering are illegal) and those consequences can be very not fun. Losing your sense of smell for months is much worse than it might sound. You do not want to get Covid-19 if you can avoid it.
Once again, these are the core things to know when forming your plan:
If we are in one of the very bad scenarios, getting the virus during the later peak will be very, very bad, and also rather likely for anyone not either immune or taking lots of precautions.
If you can work from home and otherwise take ‘reasonably careful’ precautions, you will probably not get Covid-19 even in those bad scenarios. Even in the worst case where 75% or more of the population ends up infected. But you need to prepare to take those precautions and sustain them for months, and prepare to pay that price.
It is worth securing your supplies in case the supply chain becomes an issue. The earlier you do that, the more measured you can be doing it, and the better it is for everyone.
Unless you are immune, at some point, whether or not you decide that point is already here, there is a high chance you will want to start taking extreme precautions. Be ready. If you have to choose, better to take your necessary risks now, rather than later.
I’ve said what I feel that I can. I will note that the incentives involved strongly restrict the things I can say here, whether or not I believe them – so you’ll need to work that out for yourselves.
As always, I encourage you to form your own model of the world, think for yourself, and do what you believe is right.
Two Dose, One Dose, Who Knows, You Knows
This week’s crisis is getting shots into arms before the shots spoil, but soon the limiting factor will (I hope) be not having shots to put into arms. Luckily, there are several good ways to help with that, the tricky part is getting those in charge to listen.
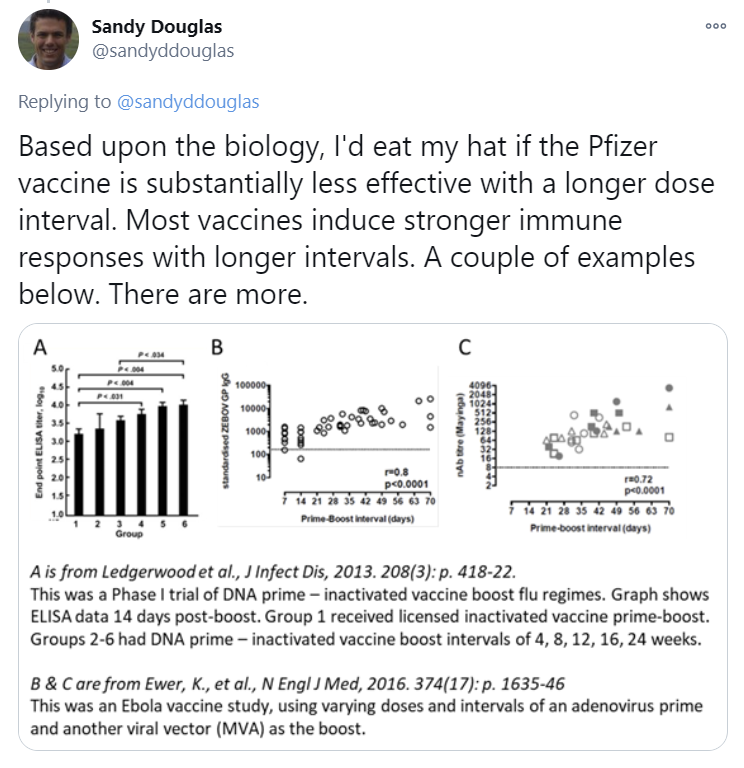
The British approved the Pfizer vaccine, they approved the AstraZeneca vaccine, they moved to first doses first and now they are allowing (not yet encouraging they are running a trial) mix and match. Under the present circumstances, the British focus on doing what it takes to save lives is smart, admirable, and impressive.
As I wrote on Dec. 10, in Herd Immunity is Herd Immunity:
Mix and matching has two potentially good properties. First, mix and matching could make the immune system response stronger than either vaccine alone because different vaccines stimulate the immune system in different ways. Second, it could help with distribution. It’s going to be easier to scale up the AZ vaccine than the mRNA vaccines, so if we can use both widely we can get more bang for our shot.
Addendum: The CDC is projecting 80,000 COVID deaths in the United States over the next three weeks.
(I included the last line because I wanted to note that this is 3,809 deaths per day and the average had not at the time been over 2,700 for any 7-day period so far, that that projection was made on December 31, so that seems like a rather bold prediction if it’s meant to reflect a physical reality rather than being a scare tactic. I can only conclude that it isn’t.)
I do think there is a legitimate worry with people’s faith in the vaccine process if you start mixing and matching, even though I expect mixing and matching to work at least as well as not doing so, and probably better. If you can pull it off without that issue, wonderful, definitely do that. Hell, at this point, anything that is clearly oriented to life saving based on modeling the physical world is something I would welcome even if I think it’s wrong on the merits (up to a point, if it’s sufficiently wrong then no that’s bad and please stop). It’s rough out there.
First doses first went from crazy two weeks ago, to the British are doing it a week ago, to now first doses first plus mix and matching.
It gives me hope, you love to see it.
I’d also like to point out that the British did a great but hard thing, closing schools exactly one day after opening them even though doing that made them look superficially like the complete and total idiots they are:
Quite right. Changing your mind and publicly admitting you are wrong, opening yourself up to blame from all sides, is hard, and should be applauded, and also there should totally be lots of screwups and reporting errors if we are moving fast enough. Good calls all around.
This is the most recent Marginal Revolution argument for first doses first. A key insight worth repeating is that there have been zero known expected value calculations in support of not doing second doses. There’s a lot of haphazard arguments and fear, uncertainty and doubt, but nothing I find remotely compelling, or that comes with any plausibly compelling numbers attached.
Allow us to present a very clean intuition pump:
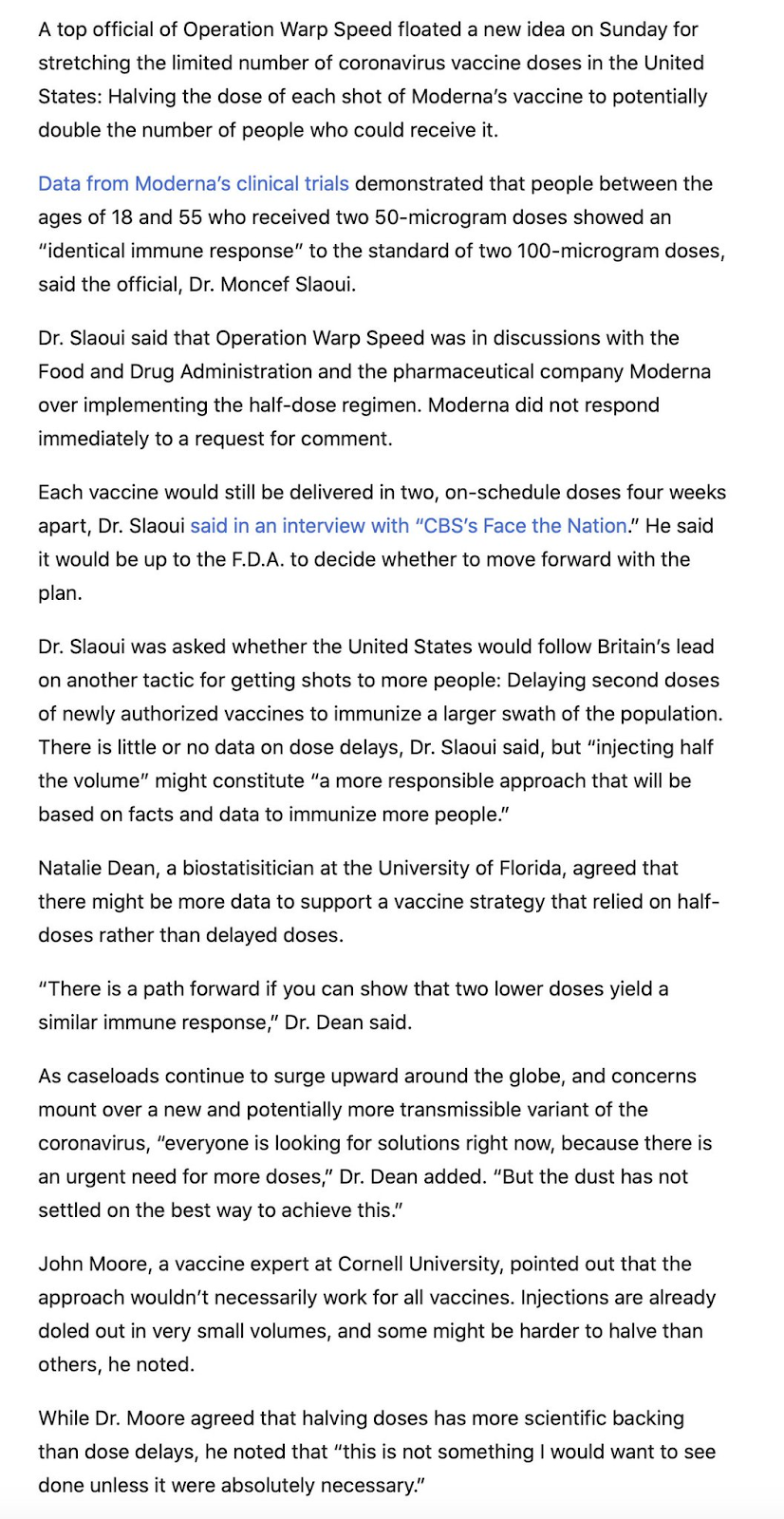
Even Operation Warp Speed is feeling enough pressure to get creative. Since there are huge low hanging gains everywhere, there’s room for different countries to find different fruit. For example, did you know that the studies seem to show half doses work as well as full doses for the non-elderly?
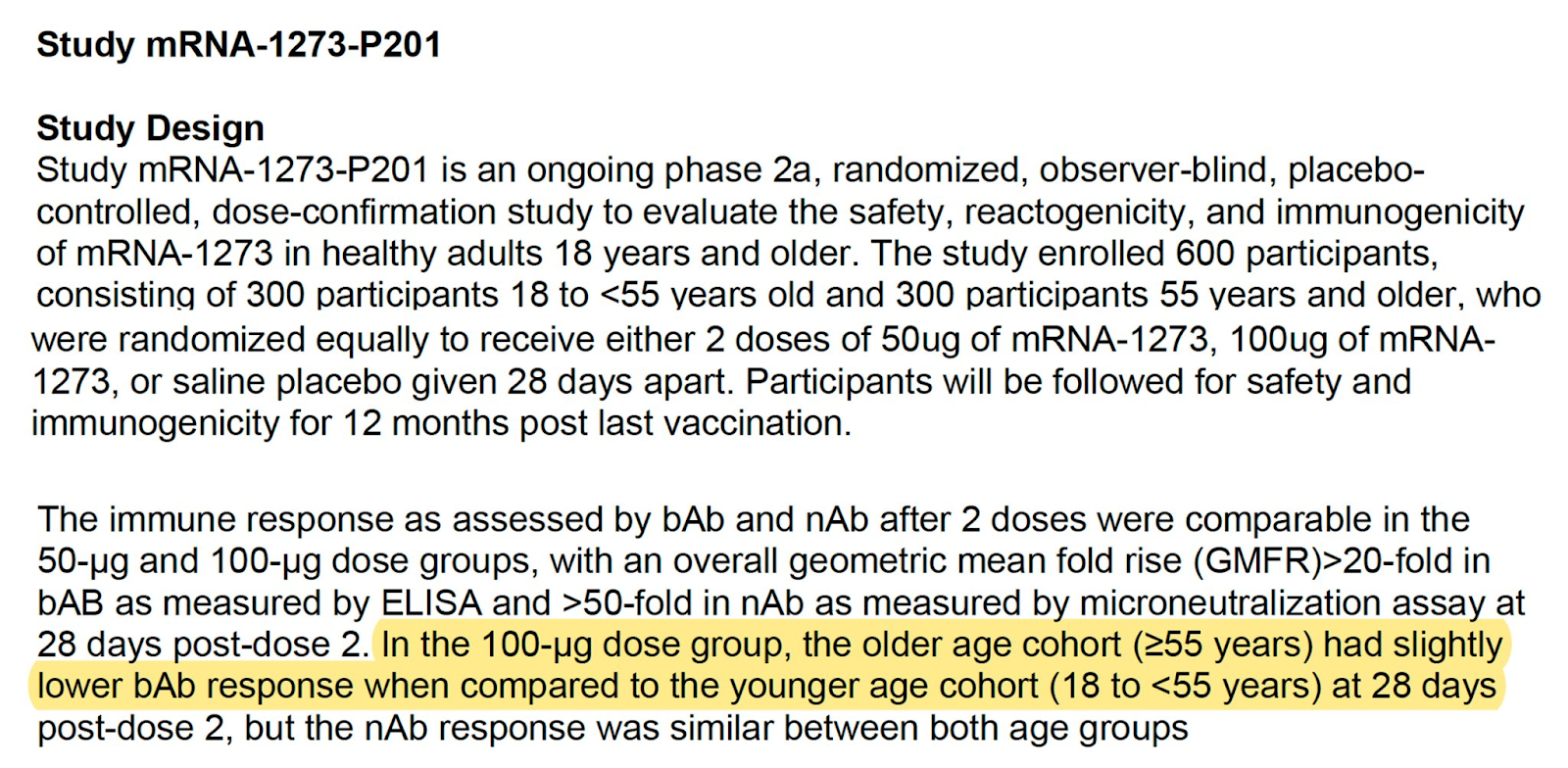
So, crazy idea, maybe give them half doses?
This thread breaks down the data available. Key findings:
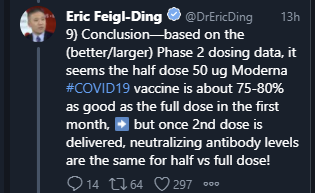
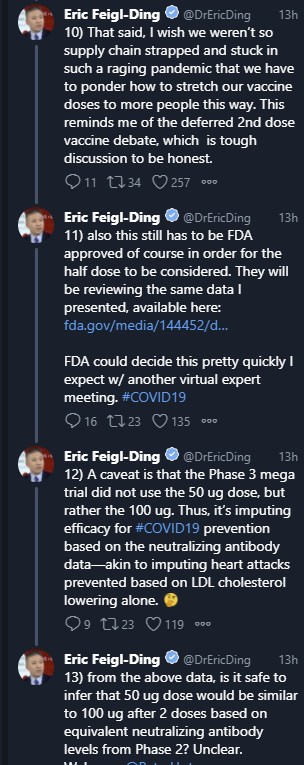
Here’s another thread, I’ll focus on takeaways.




And then there’s this, which suggests that half doses might already be way more than we need although I haven’t examined the data involved:
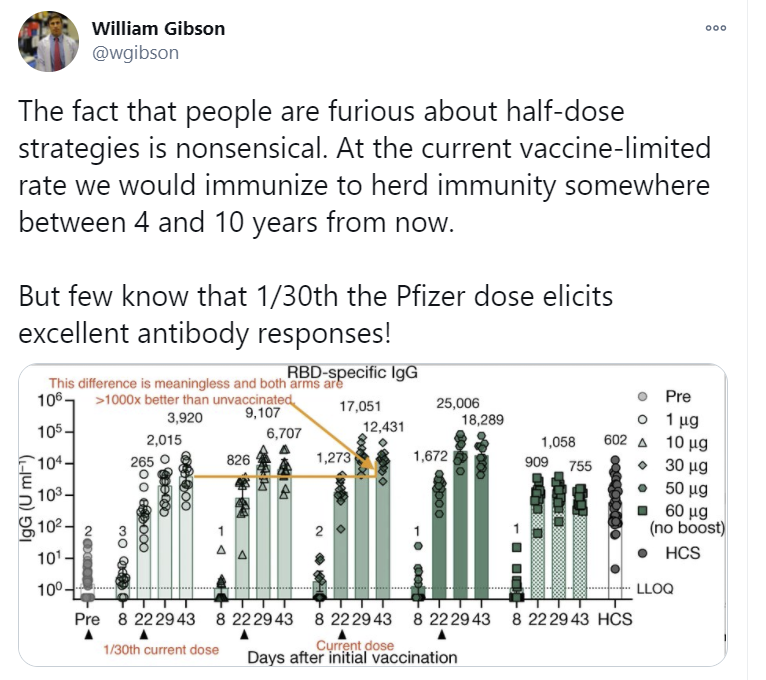
I always find it strange that people say things like “we don’t know whether a single dose vaccine provides protection from severe Covid” in spots like this. I don’t see a plausible physical way for it not to.
My conclusion (at least for now) is that the half dose is probably all you need if you are not elderly and get the second shot afterwards, with close to full effectiveness, and is more efficient per vaccine dose if given as only one dose but less effective than one full dose. There is some danger that the dropoff in effectiveness is bigger than we think, but not so big that we could plausibly come out behind on the deal. If one shot is already 80% effective, I find it highly implausible we wouldn’t do better than that with the double half-dose, given the data here.
Meanwhile, on the matter of first doses first, I’d offer to eat my hat as well, except that’s a one sided bet and also I don’t own a hat:
And everyone’s entitled to their opinion:
That all works for me. Yes, we could do so much better if everyone did all the right things and grabbed all the multiplicative low-hanging fruit, but even grabbing some of the fruit, even different fruit, is a huge win. I’ll take it.
Yes, We Can Agree Andrew Cuomo Is The Worst
That’s less true now than when I wrote this, “because of reasons,” but still. Somehow he has topped himself. I’m not saying History’s Greatest Villain, or even clearly this week’s greatest villain – the competition’s been stiff lately – but it is not through lack of trying.
On January 4, doctors outside of hospitals became eligible. On January 11, home care workers will become eligible. At some unannounced point after that, maybe we’ll get to phase 1B, which includes those over 75 years old. One hopes.
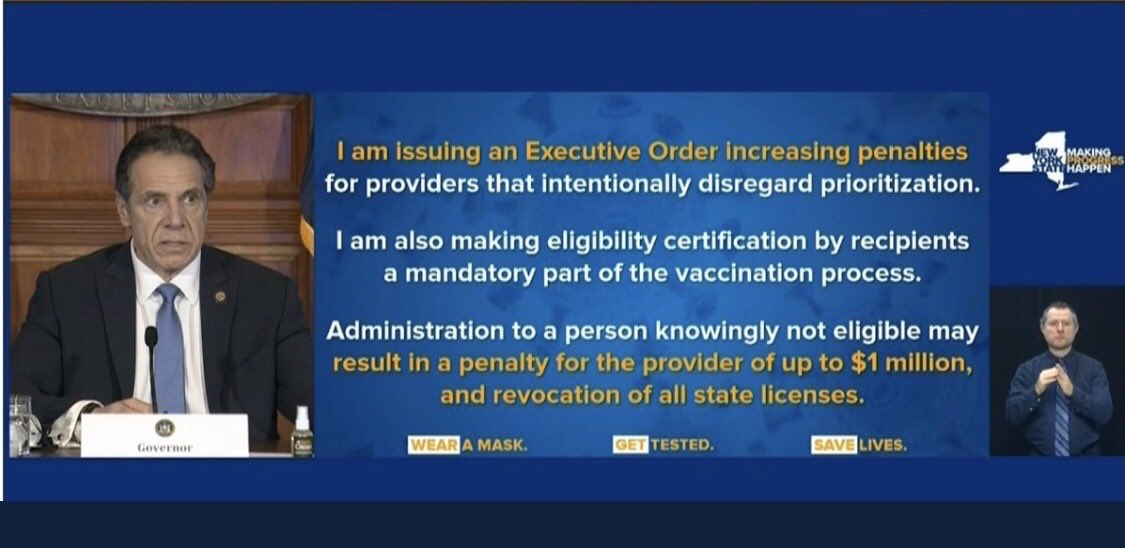
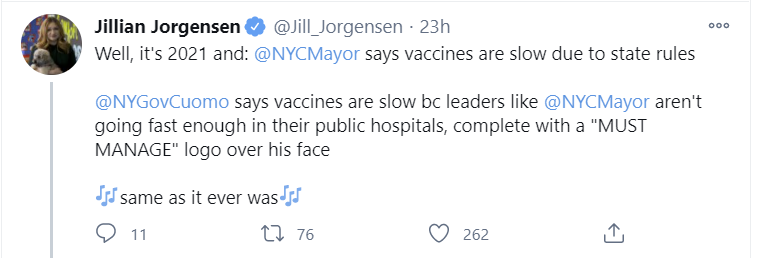
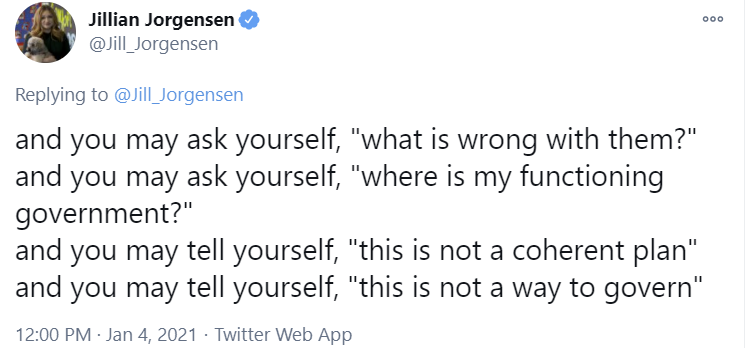
But, Cuomo says, I also threatened our health care providers to speed things up, doesn’t that fix everything?

Did you know that the more you yell and threaten, the more everyone does what you want?
Second-worst person New York Mayor DeBlasio is not happy about the threats, calling them ‘just arrogance’ because he can only think about status implications rather than physical consequences.
Oh, it’s so much worse than that. What happens when the central planner combines threats to those who don’t distribute all the vaccine doses they get, with other threats to those who let someone ‘jump the line’? Care to solve for the equilibrium?
Here’s a new framing to help you out:
Eliezer got this one wrong, because actually there is a particular nothing that will not get ruled out.
Things we will totally do in the future, to avoid the risk that someone somewhere is using our existing private infrastructure, but we’ll worry about the logistics for this when the time comes:
Note that Cuomo is not using the present tense. He is not saying “We are recruiting” such people, or that we “are establishing” such locations.
Avoiding blame in the next two weeks, you see, does not extend to problems we will have three weeks from now. Worry about tomorrow, tomorrow.
Even if you pull it off and thread the needle, it does not seem that ‘use 99% of your allocation while we have more doses than we can use despite obeying all the restrictions’ leads to the next step of then maybe you should send those places some more:
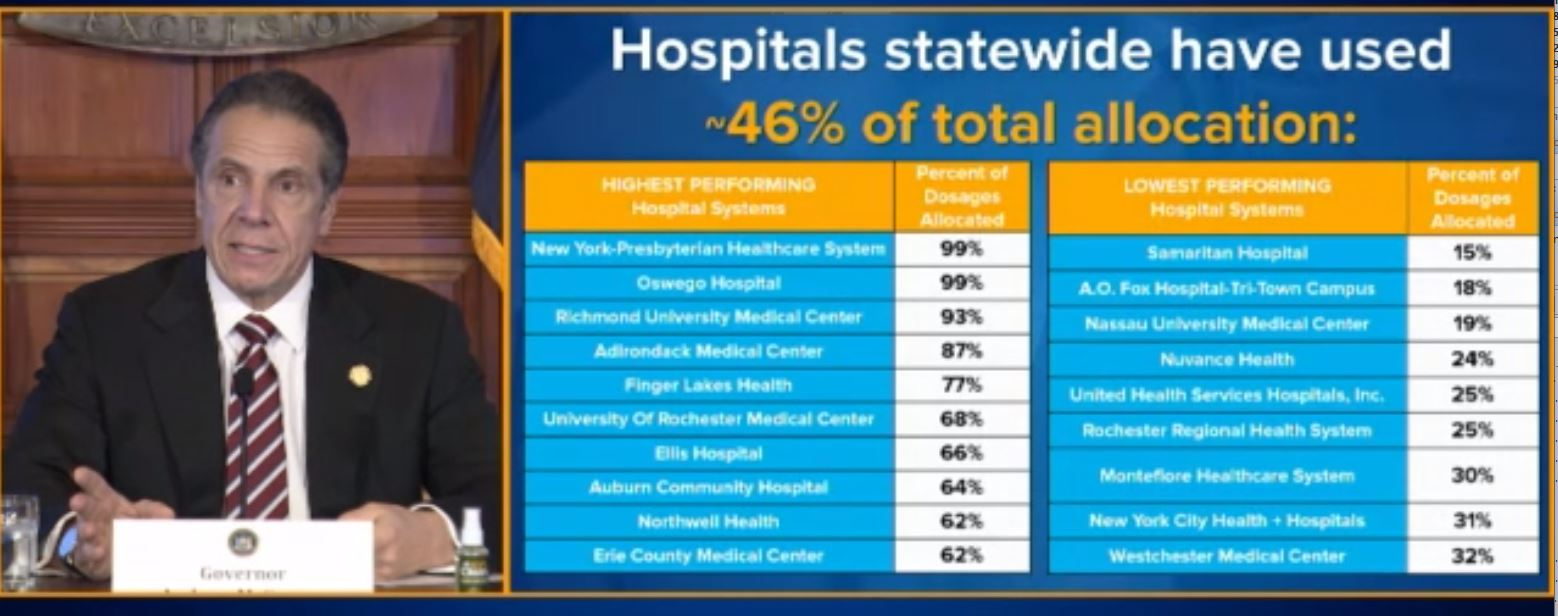
From the same thread, I’m trying to figure out the logic behind this one if it isn’t purely sacrificial, and it’s a thinker:
You have to be sympathetic, though. These logistics are hard. It’s not like there was any warning that such problems were coming. Yes, we did know vaccine shipments were likely, but it’s not like there was any time or way to plan for mass vaccinations in advance.
Oh. Wait..(you might want to read the whole thing on this one)

So let me get this straight. New York State has a detailed mass vaccination plan, developed well in advance for exactly this situation. It’s ready to go. There are distribution sites, officials in charge in each locality, every county is standing by. The plans are submitted. And we’re just going to… not use it, because we’d rather be sure that the doses all get distributed in exactly the right order.
Ross Barkan has similar thoughts about the whole mess, and offers some reminders about Cuomo’s past performance.
Even if you think there’s rhyme or reason to the decisions being made, they’re not only not transparent, they’re not being told to anyone.
No one has any idea what is going on, who has priority over who or when anyone can get vaccinated, or how and where and when one might go about doing that if you aren’t living or working at a location doing the vaccinations. No one can plan.
This is all hitting on a personal level, on multiple fronts.
As a concrete example, my wife is a psychiatrist. On Monday, she was informed (with no warning) via various roundabout methods, that she was eligible for vaccination.
The announcements said nothing about how to go about getting vaccinated, by appointment or otherwise. So we thought about what to do and she started making phone calls. A lot of phone calls. Officials directed her to other officials. Officials said they learned about the new eligibility that day the same way we had, and they were scrambling and would have to call us back. No one could provide any clarity.
After all the phone calls, she’s on one list where they will maybe call her back and offer her an appointment somewhere at some point with some amount of notice, none of which can be specified, and then she’ll need to drop everything and take that opportunity, since there might not be another. Then there are the other potential locations, which haven’t even gotten that far, and pretty much everyone has a limited supply available and also no idea how to use it.
So despite being eligible for vaccination, and despite there being lots of unused doses, and despite our willingness to get into a car and drive quite far and make a lot of phone calls, still no vaccination and no timeline for getting one.
Meanwhile, I talked to my father, who is both very old and has comorbidities. He is therefore in “Group 1b” which includes 2.5 million people in the city of New York, behind a huge pool of people in 1a who are mostly not at high risk and that are only half done, and to which groups are being added haphazardly – which makes sense, since Cuomo won’t let anyone from 1b get vaccinated, so it’s vital to expand 1a as much as possible so vaccine doesn’t spoil. When we go to group 1b, he fears slash assumes it’s going to get prioritized to go to ‘harder hit’ zip codes and areas, and that he’ll effectively be behind a quarter of the city and forced to wait, and that nothing he can do will change that. I don’t expect this and told him he was quite wrong, that the system is more than sufficiently a giant mess that being willing to call around and go where you need to go will be quite sufficient to be early in 1b.
But at this point he expects allocation by Politics and Power to do its best to kill him.
Contrast this with the system effectively being used in Florida, featuring such horrible blameworthy actions as finding ways to do things, and to vaccinate seniors who actively want to get vaccinated:

What about teachers? Good question. Who counts as an ‘education worker’ here?
What are we going to do about prisoners? Different people get different messages, so no one knows anything.
Then when confronted about having sent contradictory messages to different people, they denied everything and moved on to Cincinnati:

So it seems like we’re debating whether prisoners should be in the same tier, with effectively higher priority, than my very old, very high risk father who has effectively been under house arrest since March, and who would happily give up quite a lot to get it. Are they more deserving? Is he not at much higher risk? What the hell is this?
Except we’re denying we’re debating that because one could be blamed for either decision, and the need to decide is more than two weeks in the future, so we’re not going to decide (or at least not tell people the decision) until the last possible moment.
Do you have any idea how enraging this is?
And of course I’m way behind all those people and who knows when I’ll get a chance.
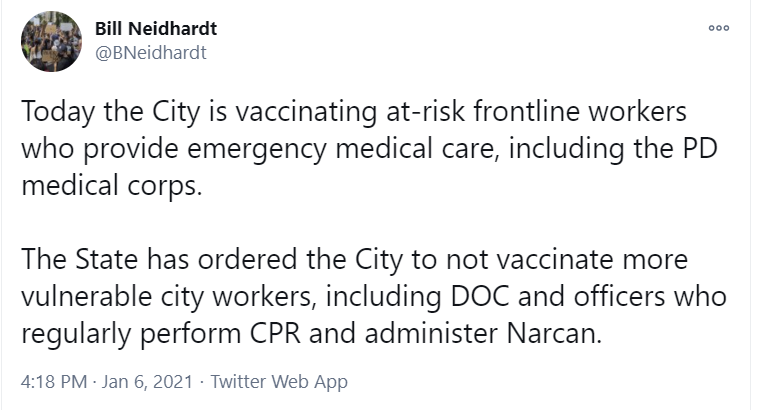
Even DeBlasio is declaring his intent to get our collective asses in gear, vowing one million vaccinations in the city in January. The problem, of course, is that he’s not allowed to do that yet, and who knows when he will be allowed (see: Andrew Cuomo is the Worst):
From NY Times via Nate Silver, so no link (Scott Alexander situation remains unresolved):
This could not be more explicit. We cannot vaccine people because there is no one we are allowed to vaccinate.
So of course Cuomo fires back:
Letting the days go by, letting the virus keep you home…
Cuomo’s not going to stand for this kind of undermining. Respect his authoritah:
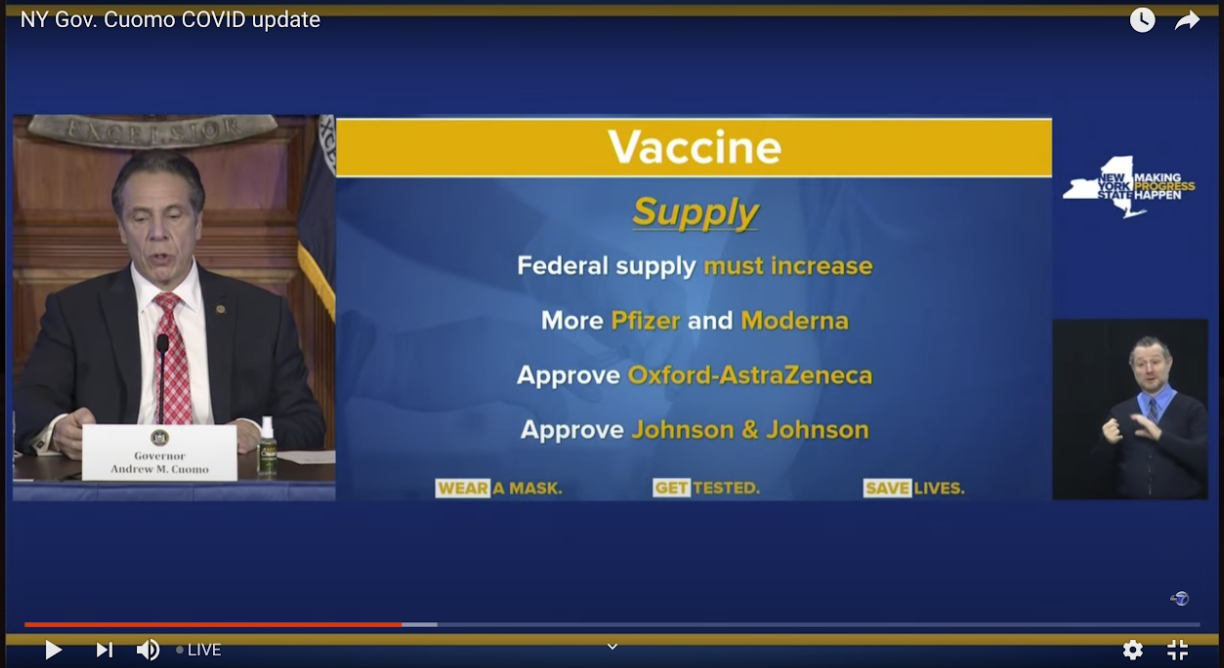
To his credit, thanks to his motivation to shift blame to the Federal Government, Cuomo is at least yelling at those responsible for getting us more supplies to get us more supplies, and to approve more sources of supply, all of which are fine things to call for, but also cheap talk:
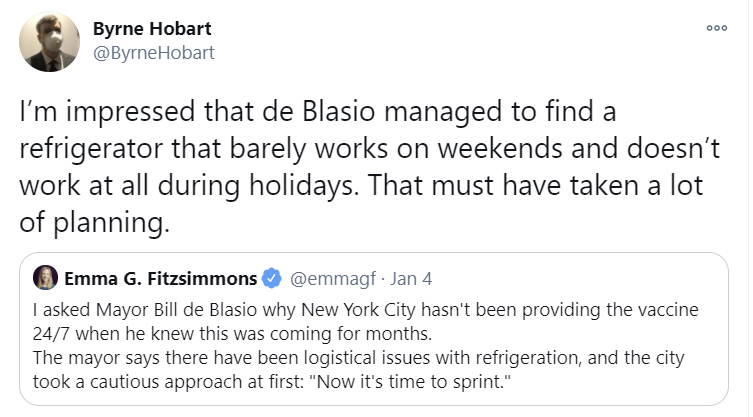
And DeBlasio does have that minor issue that the city that never sleeps does almost no weekend vaccinations, making excuses seem rather weak
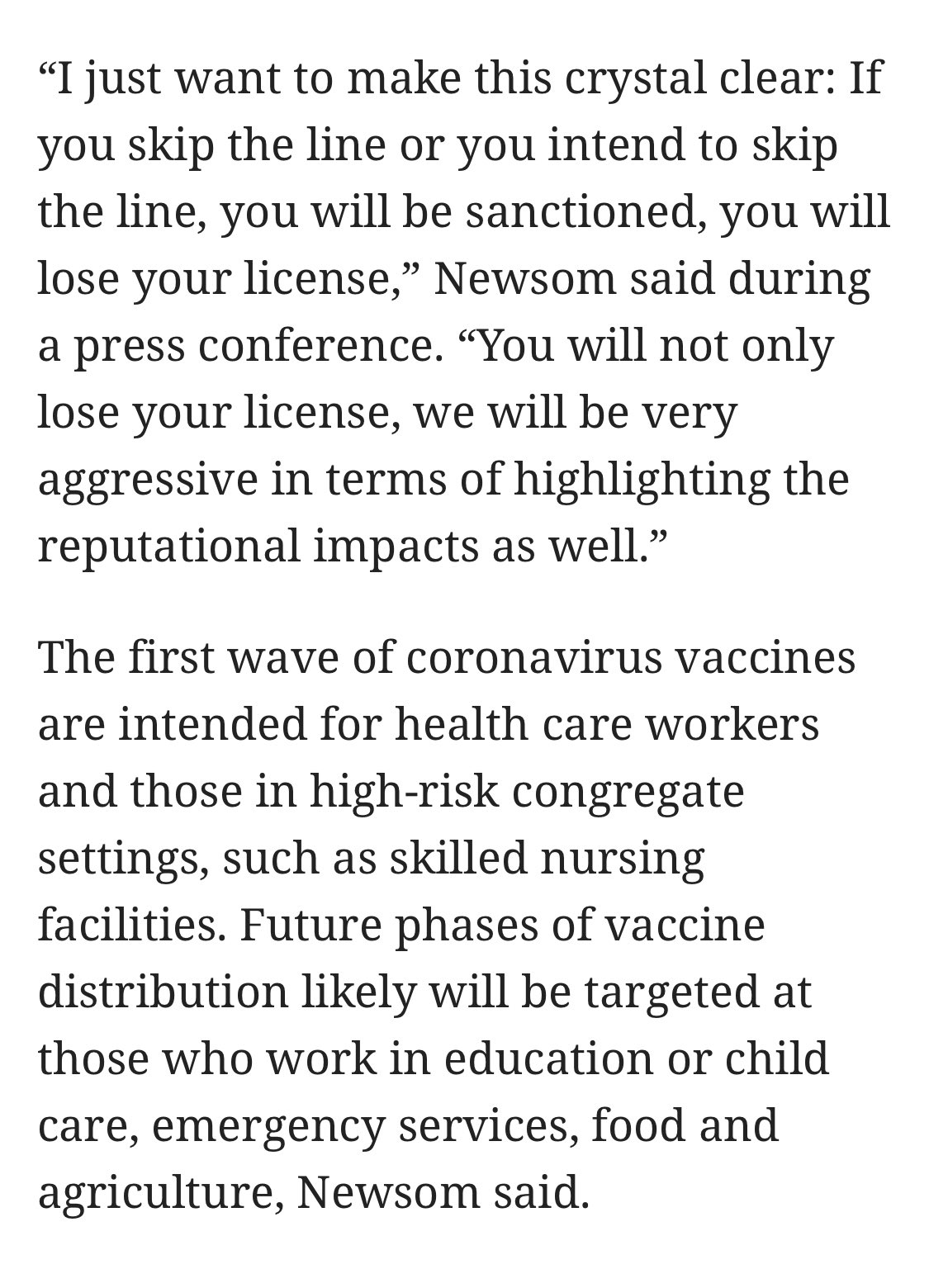
Not Cuomo, but to cover bases mentioned above, here’s the quote from Newsome, who is trying but can’t hope to compete with the champion:
Perhaps he was mad about these horrible people?

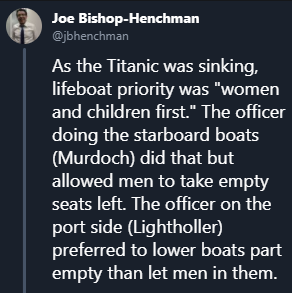
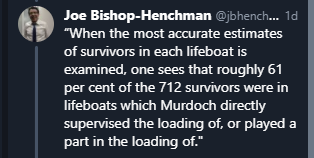
Detailed story of the evacuation is here.
In other New York news, I’d note that policies like this might have made sense back when New York’s infection and death rates were unusually low, but make very little sense now:

Although I am glad to see this which seems worthwhile:

Also, did I mention the inevitable yet?
All I Want For Christmas is a Covid Vaccine, But They Somehow Underpriced Them So Much No One’s Even Bothering To Sell Out
Israel’s approach is personified by the Pizza Guy:
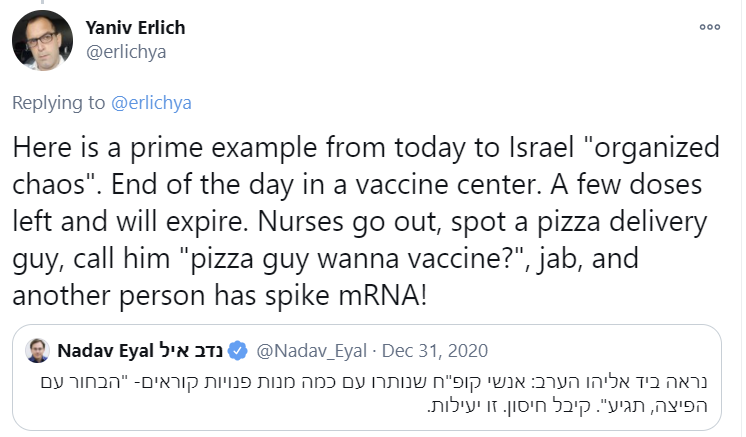
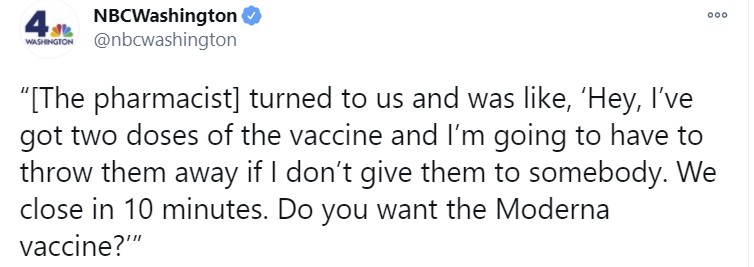
Ours, not so much.
To be fair, it does seem Washington, DC managed to get on that page, at least once, to go with the previous incident in Kentucky. This taking place in the city that isn’t part of a state seems like it might not be a coincidence, although it is also where there is a lot of media.
Then there’s the natural experiment we ran in California (source article here).
What happened was, they lost their freezer, so they had 830 doses and two hours to distribute them. They made the (obviously overdetermined and correct) decision to vaccinate as many as possible regardless of guidelines.
They still tried to prioritize:

Also, this just raises further questions:

If the doses were spoiling, could they be ‘returned’ to the county or not? If they could, why didn’t they return all the doses? If they couldn’t, how did they return 200? Was there exactly that much space in their freezer? What storage facilities were available in Ukiah?
They also didn’t skip over the issue of proper consent or a ‘safe protocol’, and prioritized on that basis:
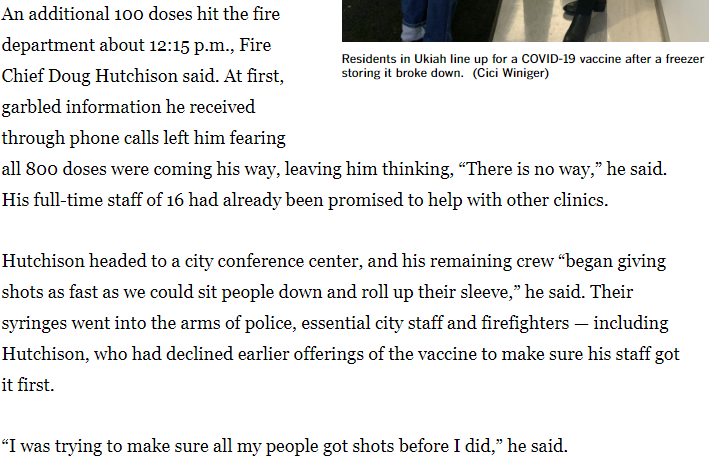
The fire department figured out how to handle a true emergency, as one might expect:
In the end, success!
Of course, then the conspiracy theories started flowing, because the freezer breaking let those with local power direct doses to wherever they want. I’m confident that didn’t happen, but I understand the instinct to think that way.
Regardless, do read the whole thing.
The conclusion is clear as day. If we cared about distribution of the vaccine, the vaccine would be distributed. Period.
The chorus rises up, and speaks as one: Shots. In. Arms. Now.
The most obvious suggestion is to maybe use the pharmacies (WSJ) that already administer the flu shot, and let them do this one in the pharmacy as per normal (MSNBC) rather than only contracting for helping with long term care facilities? Still blows my mind this one is hard. Which, in good news seen later in the week, could be happening sooner rather than later, if nowhere near soon enough.
Scott Gotleib, former head of the FDA, making multiple modest proposals, not only suggesting pharmacies administer vaccinations, but also that we administer more vaccinations:

It’s deeply sad that we need to use the language of ‘high-risk Americans have access’ to suggest using our actual existing distribution system for the purpose of distributing the things they normally distribute.
Even if we do the second shot on schedule, surely it’s madness to hold back the doses for it rather than count on future supply, right?
Yes, if the first shot doesn’t do anywhere near what we think it does, and we face a sudden and total supply collapse, then we are slightly more screwed with first doses first.
Options that exist in theory but somehow not in practice, an ongoing mystery:
Look, I totally get that nursing home residents need to get medical histories and such before you can clear them for the vaccine, but the health care workers are literally at exactly the places you give the shots and the nursing home residents are kind of there because they can’t ever be anywhere else, so who exactly are the unchallenging groups? And if it’s too difficult can we then open up the criteria a bit? No?
And yeah, how about you start scrambling and thinking about that wall that you’re going to hit BEFORE you run into the wall?
Given, Dr. Jha, that you outright said you’re going to hit that wall.
Meanwhile, the wall we’re in now:
What having a chance of being sufficiently cynical looks like:
This is beyond fully endorsed:

This as well:
Take the following tweet far more seriously than you think:
This is not mainly about Bill Gates being better than the government at logistics. This is because if the vaccine was being given with bad intent, then there would be no danger of motive ambiguity, and those with power could safely make better choices rather than worse choices.
Also I have no idea why Mark Primiamo is even half-joking:
Here’s to the courage to admit when one is both correct and isn’t joking and also everybody knows this already:
Texas does reasonable thing, and opens up Phase 1B which includes everyone over 65, which should be sufficient to find arms in which to put shots as needed:
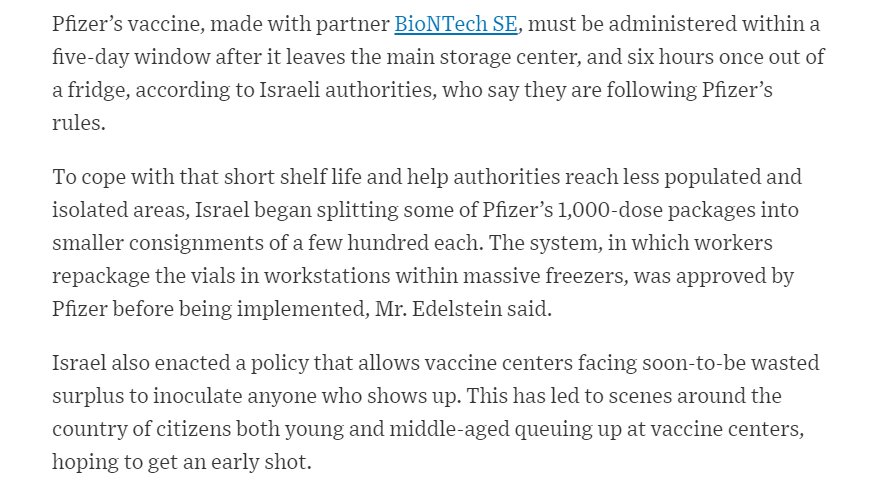
Meanwhile, in Israel, where they seem to care about vaccinating people…
Current general mood about the whole thing:

What have you to say in your defense, “ethicists”?
OK, that’s not fair. The American medical system is not Andrew Cuomo, but what would be fair?
We could… quote the FDA’s statement in full so there can be no misunderstanding?
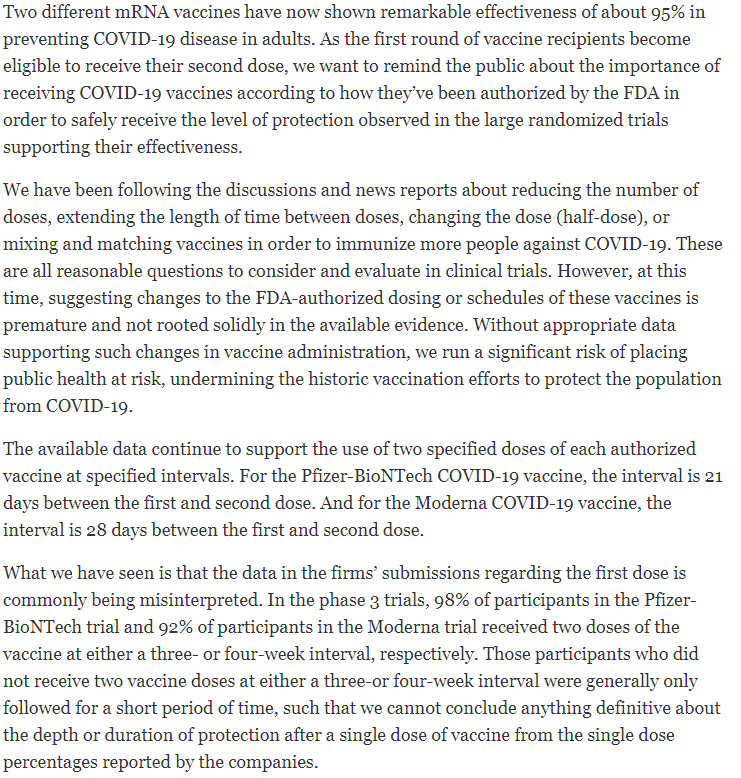
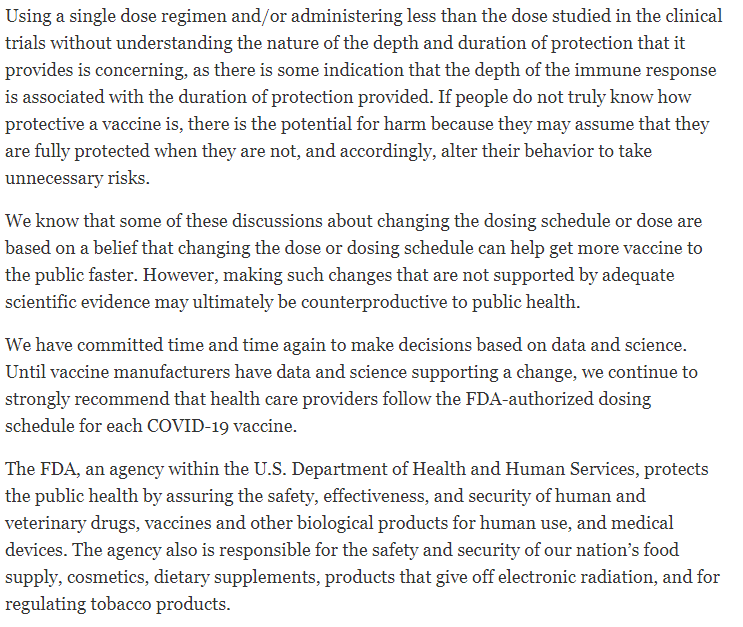
In other words, ‘data and science’ that do not exactly conform to standards don’t exist, so until you file the proper forms representing the properly numbered trials, in triplicate, we are not going to schedule a meeting for a few weeks later to consider your proposal to prevent more deaths rather than prevent less deaths via the use of these mysterious things you call “Bayesian evidence” and “logic.”
And yes, I think that is all entirely fair.
FDA delenda est.
Any defense beyond that and the response to it are going to fall under “Something Is Wrong On the Internet” so feel free to skip this section, but it seems like it should be written anyway.
This seems like the line of defense for those who aren’t going to fall back on the pure ‘it is forbidden’ and bury their heads in the sand like ostriches until someone does an RCT. In advance I admit I may be unfair here, but this seemed like a relatively thoughtful version to me, while being illustrative of the fallacies involved:
She then links to this study and this other study, which are models that conclude that vaccinating old people before young people results in more infections and less deaths, whereas vaccinating young before old does the opposite. The second, to its credit, points out that there are other considerations than a pure count of deaths, and it’s not obvious the optimization target of public policy should be purely deaths prevented – as one comment pointed out, there’s a reasonable case that QALYs saved is a better health target even if you ignore economics.
Which all makes sense, and I do buy that elderly vaccinations first minimize deaths, but only if you assume that both scenarios vaccinate the same number of people.
So it doesn’t address the question in a useful way. She goes on this way:
The third tweet illustrates the core issue. She is thinking of the alternative as ‘sits on the shelf for a week’ but that all the vaccinations still happen a week later.
If we all had confidence in that, there would (I presume) not be this chorus of panic and outrage. The problem is that we are literally worried the vaccines will expire and be thrown out, and the whole timetable will be thrown off, and it will be a huge disaster on every level. Which I’m presuming she would agree, if it were to happen, would be a huge disaster on every level.
And also that, by saving the extra dose, we would give a nursing home resident a dose when they would otherwise not have gotten one. Which doesn’t even parse for me at this point. When it comes to nursing homes, supply is not even an issue. When you are administering 20% of your doses after several weeks, returning the excess supply does actual nothing. The bottlenecks lie elsewhere.
So while I’m very confident that she’s right that it’s worth waiting a week if it transfers the dose to a nursing home resident that would otherwise have to wait a long time (e.g. a month or more), I don’t see how that has any bearing on our current reality.
The whole thread also illustrates the general assumption, by those who think we can do central planning, that we should treat the ‘baseline scenario’ as being able to allocate the way the planner wants, with no waste, no delays, no additional costs, no regulatory capture, no corruption, no allocation by politics and power that does something different from their policy paper, no perverse incentives causing strange destructive behaviors, and so on, when the actual ‘baseline scenario’ is to assume you get all of that.
No, you in practice mostly can’t usefully return excess doses, and that’s not going to change. There are lots of logistical and storage issues. And more to the point, once you allocate doses to an institution, what the hell did you think was going to happen? That they were going to give it back to be reallocated no one knows when to nowhere they’re associated and nowhere they’d get any credit, denying it to their employees and allies, rather than allocate the doses via politics and power to their employees, allies and associates?
That they’d spend their own resources to find a systematic way to quickly find people who fit into remarkably strict categories, to whom to give, at their own time and expense, completely free shots, taking on all the liability involved, including threats from the government for criminal prosecution if such people turned out not to fit the criteria?
And you also want, in that last tweet, to put (at least some of) the burden on these random institutions to then allocate the vaccine based on who has suffered disproportionately? While also obeying all the official restrictions or else, and also when did that become a priority?
If we lowered the thresholds at least to something reasonably common and easy to verify, such as being Over 65, we could at least give them a chance. Right now, I really, really don’t know what you were expecting.
Vaccine Allocation By Politics and Power
I keep hearing that nurses are actually unusually likely to refuse the vaccine, with the usual explanation being that they know all the things that can go wrong in the medical system:
It seems that nurses’ unions are taking stands to prevent the shots from being mandatory. Which takes away the whole ‘people can safely use the medical system’ advantage of doing health care workers first.
Luckily, nursing homes, where the most is at stake, seem to have it less bad.
Nursing homes seem to have reassuringly low refusal rates. 90% acceptance is not so bad.
Fluent Cherokee speakers eligible for the vaccine. If we had only known this earlier, would a bunch more people be fluent in Cherokee by now?
That one time in DC when they managed to get expiring vaccines into random people’s arms was good. Any idea why the vaccine was about to expire?
I think that’s a bit harsh there by Shoddy. More precise would be they instinctively avoid being seen as taking actions which could plausibly be interpreted as motivated by getting people vaccinated. If they had a choice, they would totally want people to get vaccinated! But they sense a grave danger if the primacy of that motivation on their part were to become common knowledge.
Thus, they can take actions that are motivated by avoiding blame for a lack of vaccinations within the next two weeks or so. They can take actions to avoid blame for vaccines actively going into trash cans. What they cannot do are the things one would do if one wanted to maximize the number of needles that get put into arms.
Thus, restrictions on who can take appointments that are so harsh that a majority of appointment times are unclaimed, rather than open up to the next tier to ensure enough demand, or allow lower tiers to make appointments on shorter notice – e.g. if the simple solution is unthinkable, how about only those in Tier 1A (whatever that locally is) can book two days in advance, then it’s opened to Tier 1B the day before, and Tier 1C same day, and you can be put on their waiting list? Or a line outside the building (at whatever tier of eligibility), and if there’s an empty slot, first come first serve?
Because I’ve certainly learned my lesson and I’m not at all bitter about it or saying I Told You So over and over again in great detail:
Another problem is that if something goes wrong and some doses get spoiled, which is something that will happen, who knows when you can get more of them?


I found this interesting in particular:

They were planning to do all residents and some staff, then lost doses, so they did some residents and some staff. Sounds like some staff (and perhaps some residents) had local political power to steer allocation, and others did not.
And of course, refer to much of the section on Andew Cuomo, as I’ve moved the rest of the New York examples over there.
How Bad is it Out There Right Now?
Pretty bad (this is from Southern California):
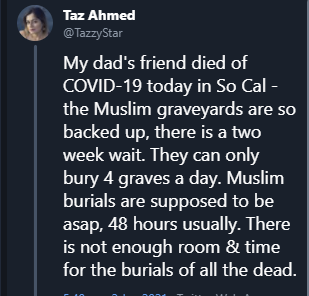
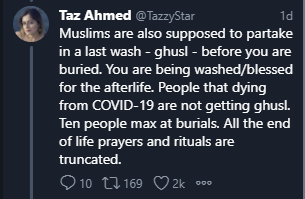
That was a few days ago, now the headlines from LA are getting much worse. We have reached full triage mode:

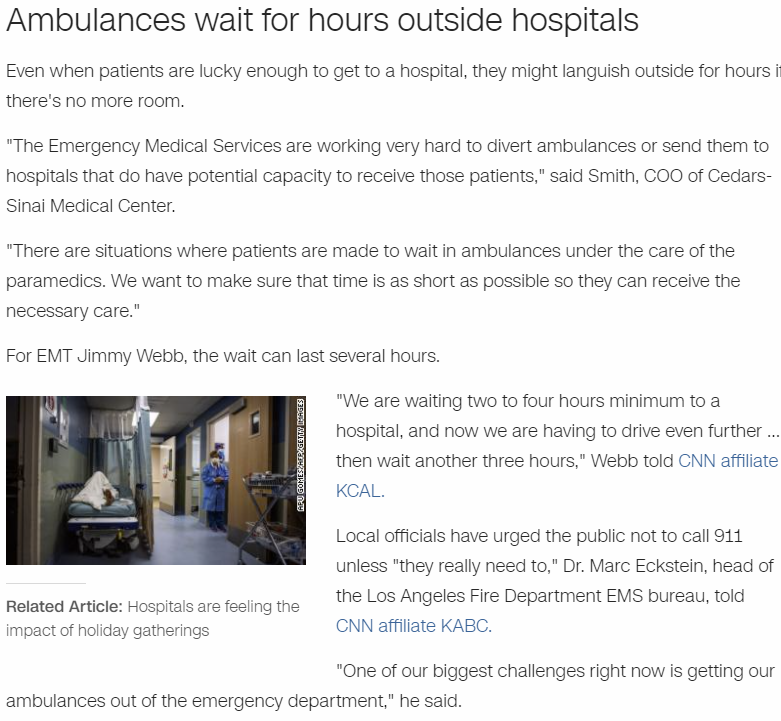
Hopefully we are very near the peak of how bad things will be this wave, but that is unlikely to be true in at least some places.
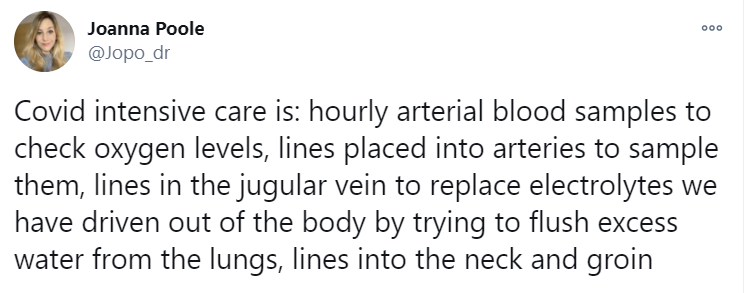
A thread on what it’s like to be treated for Covid-19, first tweet below.
Even the paper itself is not safe:
A study out of the Ohio State University from September (I looked for it and couldn’t find a reference in past weeks, but I could have missed it) finds that 30% of student athletes who previously had Covid-19 had heart damage linked to Covid-19. The whole thing is surprising not only because it means that athletes at the Ohio State University had hearts to begin with (Roll Tide on Monday!), but also because it means that they did useful work at Ohio State, it potentially interfered with their athletic department and they still published. It all makes so little sense. My model of the world can at least take comfort in knowing that this in no way actually interfered with anyone’s athletic operations.
From a tweet on the source thread that would not like to get broadcast too widely, not verified at all:

I don’t expect this to turn out to be a big deal, but I could easily be wrong and am choosing not to do the research, so if the evidence indicates otherwise, please speak up and explain.
Hospitals are not collapsed as such, but things are very much not good:
So, I guess this might have happened, with 44 cases at the hospital:
In Other News
Off-topic but awesome: Money Stuff is back! Matt Levine returns from parental leave with the best daily newsletter I have ever known, and it is not remotely close. This is about the latest happenings of all things money, hence the name, but written in such a way that it appeals both to professional traders and to people who don’t otherwise know or care about money stuff. I’ve been known to read the column out loud to my wife, without having read it first, and it’s reliably both funny and enlightening. The perspective you get here is not the whole picture, but your picture of the world without it will be incomplete. You can fix that. Strong endorsement.
Bryan Caplan asks, have you tried… being happy this year?
Your periodic reminder that in 1947, New York City vaccinated ~6.35 million people (80% of their population) for smallpox in less than a month. If you do not think we can do this, what changed to make it impossible?
Your periodic reminder that the FDA’s incentives are bad.
What did China do to stop this virus and get back to normal? What didn’t it do? (Inessential and snarky Twitter thread)
British official report on AstraZeneca vaccine is out. As we expected, less good than Pfizer or Moderna’s in terms of effectiveness, far better than it needs to be to be worthwhile.
There’s an AstraZeneca manufacturing plant in Baltimore. It seems we’re really going to wait until April to approve their vaccine, the interpretation of which I leave to you the reader.
AstraZeneca has vowed not to make a profit on their vaccine ‘until the pandemic is over.’ They have also declared the right to declare the pandemic ‘over’ in July 2021. So due to the fear that someone, somewhere, might be earning a profit, a major corporation makes money if they sell doses after July 2021, but not if they sell them before July 2021. I wonder what they will do. (Original Hat Tip)
Every few weeks, the evidence for immunity for those who have been infected gets one week longer, and by Lindy that means two more weeks of immunity, yet I still get people claiming “we don’t know how long immunity lasts” or saying it fades after a few months, and so on. This leads to insanity like this, where in order to satisfy such folks, a star NBA player is missing games under quarantine for exposure despite having not only already had Covid-19, but having been confirmed to have antibodies:
I don’t blame the NBA either. People respond to incentives. The NBA is very well known to not be an exception to this. Trust the process.
You know who has a lot of supply coming soon? India:
If you live in the greater Washington D.C. area, there was a super-spreader event on January 6, so stay safe. Everyone else, you too.
I’ll see everyone next week. Hopefully with better news.
56 comments
Comments sorted by top scores.
comment by supposedlyfun · 2021-01-08T00:48:35.672Z · LW(p) · GW(p)
You deserve to be paid for these covid updates. Are you getting paid? How does one pay you for this? This must've taken at least 15 hours.
Replies from: romeostevensit, knite↑ comment by romeostevensit · 2021-01-08T04:00:35.084Z · LW(p) · GW(p)
Aaron Gertler [LW · GW] is helping administer crowdfunded award to Zvi for this series. You can PM him for details.
Replies from: Zvi, Kenny↑ comment by Zvi · 2021-01-08T11:13:05.435Z · LW(p) · GW(p)
That's the established way we are doing this. If you want to pay me directly you can PM me for payment details.
Money is not in any way the reason I write these posts and I've been fortunate in that I can afford to do them without being paid, but good incentives and extra cash are always welcome.
Replies from: rockthecasbah, Kenny↑ comment by Tim Liptrot (rockthecasbah) · 2021-01-08T15:10:27.779Z · LW(p) · GW(p)
The incentives run against saying things like Jay Bhattacharya has (we are causing more prevention harms than benefits). Is there a way to change that?
↑ comment by Kenny · 2021-01-14T17:17:37.598Z · LW(p) · GW(p)
Aaron gave me the details on how best to pay you but it's not info I'd publicize without your explicit consent.
I'd like to pay you, others seem to want to do the same thing, but I don't want to create extra work for you for this.
Would you mind someone setting up a Patreon on your behalf and then paying you any money collected via it (i.e. via the method Aaron shared)?
Replies from: Zvi↑ comment by Zvi · 2021-01-14T17:34:51.185Z · LW(p) · GW(p)
Unless it's a bigger hassle than I expect I should be able to do it myself, if I'm gonna do it makes sense I should learn how it works and keep control over it. It looks like they take 8% if you have tiers (which everyone has) and 5% if you don't, and then payment charges, which are 5%+ for small payments and 3% for large ones, so we lose 11% doing this, which pains me. Is this the best we can do?
Replies from: mingyuan, Kenny↑ comment by Kenny · 2021-01-15T16:53:31.189Z · LW(p) · GW(p)
You (or someone) could use a payment processor with a subscription feature, e.g. Stripe, and lose only 2.9+%.
Maybe the easiest/cheapest option would be to just create a new email address and accept direct payments via Zelle/Venmo/PayPal/etc., but some of those don't support recurring payments.
↑ comment by knite · 2021-01-09T00:30:47.216Z · LW(p) · GW(p)
I agree! I would happily support these updates on Patreon, if that were an option. I understand that from Zvi's perspective that could be problematic for any number of reasons, including possibly reducing motivation.
Zvi - since "money is not in any way the reason I write these posts", how about favorite charities?
Replies from: Zvi↑ comment by Zvi · 2021-01-09T00:35:20.017Z · LW(p) · GW(p)
To be clear, I will happily accept any contributions people want to make, although I don't currently have a Patreon, and I believe this would be motivating rather than demotivating.
But if you'd like to donate it to charity instead, that's great too and I'd ask it be given to MIRI.
comment by maia · 2021-01-07T17:41:13.236Z · LW(p) · GW(p)
Still reading through the rest of the post, but this jumped out at me. Your dad said:
convalescent sera from some patients recovered from infection with the predominant strain, while effective in neutralizing the same strain, were not effective in neutralizing the South African variant.
But you then said:
it seems highly unlikely the new strain can do much reinfection of previously infected individuals
which seems to me to be the opposite. If convalescent sera from patients who recovered from infection with the predominant strain were NOT effective in neutralizing the South African variant... doesn't that suggest that having had the predominant COVID variant might NOT give you immunity to the South African variant?
Trying to nail this down because this point is SUPER IMPORTANT actually.
Replies from: Zvi, brianwang712, TheSimplestExplanation↑ comment by brianwang712 · 2021-01-07T22:55:08.557Z · LW(p) · GW(p)
Looks like we have at least one case of reinfection with one of the new variants containing the E484K mutation (this isn't the South African variant, rather from the Brazilian lineage where E484K independently arose).
↑ comment by TheSimplestExplanation · 2021-01-08T14:20:45.359Z · LW(p) · GW(p)
Not having neutralizing antibodys doesn't mean you're not immune, or at least partially immune. People still have many antibodys against the virus.
comment by TurnTrout · 2021-01-08T17:48:37.814Z · LW(p) · GW(p)
Biden plans to release nearly all available vaccine doses in an attempt to speed delivery
“The president-elect believes we must accelerate distribution of the vaccine while continuing to ensure the Americans who need it most get it as soon as possible,” T.J. Ducklo, a spokesman for the transition team, said.
“He supports releasing available doses immediately, and believes the government should stop holding back vaccine supply so we can get more shots in Americans’ arms now. He will share additional details next week on how his Administration will begin releasing available doses when he assumes office on January 20th.”
comment by MondSemmel · 2021-01-07T23:59:09.996Z · LW(p) · GW(p)
Zvi, my heartfelt thanks once again for the herculean efforts you're going to in creating these Covid posts.
---
Tiny formatting error: The link on "even though doing that made them look superficially like the complete and total idiots they are:" points to a Google Doc that prompts me with "You need access" instead of to the Twitter image immediately below.
comment by DirectedEvolution (AllAmericanBreakfast) · 2021-01-07T22:22:57.196Z · LW(p) · GW(p)
I've been thinking about the Road to Serfdom. This debacle makes me realize that Hayek's move on the intellectual chessboard was to position government planning as an atypical "extra set of options" for distribution of goods and services beyond the "default" of market distribution on a price basis.
In fact, we can see that what constitutes the "default" is an empirical political matter. In our country, at least when it comes to medicines, government planning is the "default," and if we did distribute on a price basis, that would be a government plan to distribute on the basis of price.
Allowing and defining the scope of a market economy is fundamentally a government plan. And it too is subject to the maddening contests of planners and all the other nonsense that Hayek described. Each plan, including price-based distribution, has its partisans, planners, theorists, and activists, and each is an ox in the run of the bulls.
Although I still think that partial or even full price-based allocation could be a very good thing; as well as permitting, now, an additional price-based infrastructure alongside our current political allocation; I also think that this is yet another plan, rather than an alternative to planning.
Where the concept of "default" steps in is in how any particular form of good is typically regulated and allocated in a specific country. In our country, we have a "default" of heavy regulation and a government-led approach to crisis. We don't respond to crime waves by letting neighborhoods hire mercenaries; we don't respond to hurricanes by letting the market sort things out; we don't respond to pandemics by letting the market self-regulate and self-allocate.
The government directs emergencies. That's our default. With all the heat of advocates for this and that alternative plan, we stick to that very simple 4-word rule.
How might Hayek interpret our response to COVID, in terms of the cartoon on pg 37 of the PDF?
- Pandemic forces national planning: we gladly surrender many freedoms and know that regimentation was forced by the virus.
- Many want planning to stay: arguments for a "vaccine distribution plan" are heard before the vaccine is approved. Pandemic planners who want to stay in power encourage the idea.
- The planners promise utopias: a rosy plan for equitable distribution goes over well in leftwing areas; a plan for price-based allocation is popular among economists -- and so on. (I guess the planners are already in office, so they don't need to be elected).
- But they can't agree on ONE utopia: with vaccines, a new set of policymakers become relevant, but "get through the pandemic safely" unity is gone. The planners nearly come to blows. Each has his own pet plan, and won't budge.
- And citizens can't agree either: When the planners finally patch up a temporary plan months later, citizens in turn disagree. What the leftwinger likes, the economist doesn't like.
- Planners hate to force agreement: most national planners are well-meaning idealists, balk at any use of force. They hope for some miracle of public (or expert) agreement as to their patchwork plan.
- They try to sell the plan to all: In an unsuccessful effort to educate people to uniform views, planners establish a giant social media machine -- which the coming dictator will find handy.
- The gullible do find agreement: Meanwhile, growing national confusion leads to social media griping. The least educated -- thrilled and convinced by fiery oratory, storm the capitol.
- Confidence in planners fades: the more that the planners improvise, the greater the disturbance to normal business. Everybody suffers. People now feel -- rightly -- that planners can't get things done!
- Andrew Cuomo is given power: In desperation, New York State bureaucrats support Andrew Cuomo to hammer out a plan and threatens million-dollar fines and reputational savaging to force its obedience. Later, they'll dispense with him -- or so they think.
- Very Serious People take over the country: by now, confusion is so great that obedience to Andrew Cuomo must be obtained at all costs. Maybe you post a "In this house, we believe..." sign on the lawn yourself to aid national unity.
- A negative aim welds party unity: Early step of the Very Serious People is to inflame the majority in common cause against some scapegoat minority. In America, the negative aim is anti-"human garbage"?
- No one opposes Andrew Cuomo's plan: It would be career suicide; new social media influencers are ruthless. Ability to force obedience always becomes the no. 1 virtue in the Very Serious State. Now all freedom is gone.
- Your vaccine is delayed: the efficient distribution promised by now defunct planners turns out to be a tragic farce. Planners never have delivered, never will be able to.
- Your return to work is delayed: opening of institutions must be arbitrary and rigid. Running a planned state from central headquarters is clumsy, unfair, inefficient.
- Your thinking is planned: In the dictatorship, unintentionally created by the planners, there is no room for difference of opinion. Billboards, press, social media -- all tell you the same lies!
- Your recreation is planned: It is no coincidence that parks and playgrounds have been carefully restricted in all regimented states. Once started, planners can't stop.
- Your disciplining is planned: If your medical license is cancelled, you're apt to get cancelled as well. What used to be an error has now become a crime against the state. Thus ends the road to serfdom!
comment by agc · 2021-01-08T17:20:38.471Z · LW(p) · GW(p)
The actions would have made (some) sense if we were supply constrained on vaccines. If supply is severely limited, you want to incentivize ordering only what you will definitely use, and you want to be very careful about using each dose in the most effective way.
It seems everyone assumed we'd be supply constraint and then never updated when it turned out distribution is the bottleneck. Actually, do we have strong evidence that vaccine supply is not currently limited in the US?
One reason I'm asking is that the UK seems to be doing much better in theory: Simpler rules, mostly based on age, no silly fights between governors and mayors, not a lot of scandals. Still, in shots per capita they are only slightly ahead. Is UK vaccine use slow in a less publicly embarrassing way, or are they supply limited while the US is not?
Replies from: thjread↑ comment by Thomas Read (thjread) · 2021-01-14T08:18:30.009Z · LW(p) · GW(p)
The UK does seem to be supply limited, or at least limited on something before the point where vaccines get delivered to hospitals. They've also sped up quite a lot in the last week.
comment by Rain · 2021-01-08T14:57:32.097Z · LW(p) · GW(p)
Your periodic reminder that in 1947, New York City vaccinated ~6.35 million people (80% of their population) for smallpox in less than a month. If you do not think we can do this, what changed to make it impossible?
What changed? We started looking for every possible negative consequence of rolling out vaccines that quickly, and then working to mitigate each and every one.
comment by Douglas_Knight · 2021-01-08T04:26:48.464Z · LW(p) · GW(p)
this is 3,809 deaths per day and the average had not at the time been over 2,700 for any 7-day period so far, that that projection was made on December 31, so that seems like a rather bold prediction
If cases are in unprecedented territory, you should expect deaths to go into unprecedented territory. Forecasting deaths 3 weeks in the future should be easy, since it's forecasting the progression of the disease among people already infected. You just take the number infected of cases and multiply by the CFR. At 220k cases/day and a CFR of 1.75%, that's 3850 deaths/day, so that sounds totally reasonable.
(This is all from eyeballing 7-day rolling averages. I got the CFR from comparing the plateau of cases in September to the plateau of deaths in October. I haven't checked if it has held up or what the lag should be. The 220k cases/day is the 7-day average peak at Christmas. So this requires assuming that the dip after Christmas was an illusion, which has been vindicated by the week since the prediction was made.)
Added: over at Zvi's blog, Alexander Gordon-Brown claims that CDC does not predict 80k deaths, but that its point estimate is only 64k. Also, that the prediction is dated 12/21.
comment by ryan_b · 2021-01-08T12:59:52.335Z · LW(p) · GW(p)
It seems to me adding price allocation would make the problem much worse rather than better. We don’t have real scarcity; we have induced scarcity because the government is hoarding. A price mechanism at this point just means the rewards for hoarding are much greater, which seems like it would incentivize more hoarding. If memory serves, that is exactly how famines work.
An unrelated thought occurred to me about the counterfactual case where market distribution was chosen upfront: why don’t we consider price setting/discovery a time penalty in the same we consider identity verification a time penalty? One click buying from Amazon is faster than showing my ID, but EBay auctions are quite a bit slower.
Replies from: rockthecasbah↑ comment by Tim Liptrot (rockthecasbah) · 2021-01-08T15:06:19.968Z · LW(p) · GW(p)
The assumption of pricing policies is that people would buy vaccines from the companies, rather than the government hoarding intermediary.
Replies from: ryan_b↑ comment by ryan_b · 2021-01-08T20:03:55.586Z · LW(p) · GW(p)
In the general case, sure - but in the post it was in the context of appointments for getting vaccines under the current paradigm. Unless I have completely misunderstood, in which case I am wrong and my comment is meaningless.
Though I still like the causes of famine as an analogy for the vaccine problem.
↑ comment by Tim Liptrot (rockthecasbah) · 2021-01-10T21:07:19.690Z · LW(p) · GW(p)
Speculation on the vaccine price in a liberalized market is an interesting question. In general I would expect the vaccine price to decline as more and more people become immune around you. But given the existing cyclical structure a speculator might foresee an infection peak and horde for it. I'm sure there are historical examples to resolve the question, but I'm lazy.
comment by Dirichlet-to-Neumann · 2021-01-08T00:16:42.882Z · LW(p) · GW(p)
I have a genuine question about RNA vaccines (not vaccination in general, RNA vaccines). It's a concern about vaccine safety, and I post it hidden here because at any other place the result would be people freaking out and getting less likely to get vaccinated if there is actually no reason to be concerned.
First a bit of context. I had a conversation with a friend of my parents. He is a researcher in biology/genetic/aging at the CNRS in France, and as far as I can tell pretty good at his job (based on his career so far).
We discussed RNA vaccines, and he was saying this:
1) The Pfizer/Modena vaccine have obviously no short term side effect so we should just vaccine all old people asap.
2) for younger people it's less clear, because of the following possibility:
RNA can obviously enter the cell nucleus (that's RNA function). What is less-well known is that RNA and DNA can sometimes mix. This mean that viral RNA from the vaccine has a chance to insert itself randomly into your DNA. In the short term this is not a problem, but in the long term this means some chances to develop some sort of cancer (or sterility problems) - which may be a problem if young people in their twenties/thirties get a lot of cancer ten years from now.
In my model this is not really a problem, because the odds of developing a cancer due to the vaccine are still very low and the benefit from vaccinations are very high and immediate (and you protect others). But I'd like to know if some of you have sources on this question or have thought about the problem.
(note: he has a long experience of targeting some gene in flies and seeing some random mutations pop out on non-targeted areas - just to say that he knows his stuff about genetics).
(note 2: also thanks Zvi for your great posts !)
Replies from: jowen, Douglas_Knight, agc↑ comment by jow (jowen) · 2021-01-09T00:24:21.993Z · LW(p) · GW(p)
Above you write: “ RNA can obviously enter the cell nucleus (that's RNA function). ”
but I believe this is not true.
Normally, mRNA is produced in the nucleus and then is transported out of the nucleus. It is then turned into protein by ribosomes, which reside outside the nucleus.
My understanding is that mRNA from mRNA vaccines is not thought to enter the cell nucleus—and certainly this is not necessary for their function.
↑ comment by Douglas_Knight · 2021-01-08T18:24:33.321Z · LW(p) · GW(p)
That doesn't distinguish the new vaccines from traditional attenuated vaccines, which also inject nucleic acid into the cell, although inactivated vaccines don't. Or, for that matter, getting infected. Every year I get a couple of colds, where way more cells get way more nucleic acid than in vaccine.
Replies from: Dirichlet-to-Neumann↑ comment by Dirichlet-to-Neumann · 2021-01-08T22:27:58.206Z · LW(p) · GW(p)
That was my initial reaction too, but then I thought that when a virus enter a cell (or a traditional attenuated vaccines), it kills the cell when going out, so any mutation that could happen to the infected cell is irrelevant since the cell is destroyed. With a RNA vaccine the cell is not killed (unless it is then killed by our immune system ?).
Replies from: Douglas_Knight↑ comment by Douglas_Knight · 2021-01-09T14:49:45.940Z · LW(p) · GW(p)
I don't believe that every infected cell is killed.
↑ comment by agc · 2021-01-08T10:56:31.921Z · LW(p) · GW(p)
Minor nitpick, but it's RNA vaccines in English (or mRNA). I take it ARN is the French word order.
Replies from: Dirichlet-to-Neumann↑ comment by Dirichlet-to-Neumann · 2021-01-08T15:54:51.060Z · LW(p) · GW(p)
Thanks - corrected.
comment by Annapurna (jorge-velez) · 2021-01-07T23:31:57.327Z · LW(p) · GW(p)
Great post as usual.
I just want to update you that my sister got the first jab in UAE on Tuesday. She's in her late 20s and works from home. Literally last in any vaccine priority list.
She walked in first thing in the morning, walked out in less than 20 minutes. She will be back on the 26th for her second shot.
comment by TheMajor · 2021-01-07T22:41:27.090Z · LW(p) · GW(p)
Oh, it’s so much worse than that. What happens when the central planner combines threats to those who don’t distribute all the vaccine doses they get, with other threats to those who let someone ‘jump the line’? Care to solve for the equilibrium?
You conclude that vaccination facilities will reduce their orders so they are guaranteed to be able to distribute all. I think in practice it is much easier to cook the books and/or destroy vaccines as necessary.
More pressingly, this is the first mention I've run into of the potential seriousness of the South African variant. But (perhaps for the first time since February) it really seems to be the case that "more data is needed before we can make an informed judgment on this"?
Replies from: Zvi, TheSimplestExplanation↑ comment by TheSimplestExplanation · 2021-01-08T14:32:07.380Z · LW(p) · GW(p)
If you have the choice it seems simpler and safer to order no vaccine. Especially if you're hardly getting paid anyway.
comment by Craig Fratrik (craig-fratrik) · 2021-01-07T17:54:49.073Z · LW(p) · GW(p)
You might want to add Ireland to your Europe graph. It is now higher than UK and much steeper. Portugal is also running parallel to UK since Dec 28 (in log levels).
Actually in general, how do you decide who is in vs out? Netherlands and Denmark are still on the decline.
Replies from: Zvicomment by Jeffrey Hu (jeffrey-hu) · 2021-01-08T05:30:47.273Z · LW(p) · GW(p)
What are your thoughts on https://www.biorxiv.org/content/10.1101/2021.01.07.425740v1 for Pfizer effectiveness against South Africa variant?
Replies from: Zvi, Douglas_Knight↑ comment by Zvi · 2021-01-08T11:17:17.935Z · LW(p) · GW(p)
Will send this to my father for technical evaluation, but this looks like it is testing a particular mutation that is also in the UK variant. It's good and reassuring news to be sure, but I don't think it answers the question we need answered.
↑ comment by Douglas_Knight · 2021-01-08T19:59:14.589Z · LW(p) · GW(p)
This is about the change that is shared between UK and SA, not about the change in the SA variant that is uniquely worrisome.
comment by Zian · 2021-01-08T04:18:48.676Z · LW(p) · GW(p)
full triage mode:
The crews are instructed to stop transporting patients who are unlikely to be resuscitated. In other words, before this point, patients were being transported to hospitals for the sake of warm fuzzies, not utilions.
From the perspective of terminal values, I'm not sure if this change actually changes anything.
Replies from: Douglas_Knight↑ comment by Douglas_Knight · 2021-01-08T04:39:07.297Z · LW(p) · GW(p)
10% chance of survival is "unlikely" but it's lives, not warm fuzzies. It may not have been cost-effective, but it was buying something real. (And it may well have been cost-effective if it was marginal use of facilities that already existed.)
10% is the number I have heard for the specific category I have heard triaged against in LA, namely patients whose heart the EMT can't restart. Instead they can perform CPR to manually pump the heart on the trip to the hospital.
Replies from: Zian↑ comment by Zian · 2021-01-08T05:01:26.002Z · LW(p) · GW(p)
In the interest of not falling prey to the illusion of transparency, I must ask if you are familiar with normal hospital offload times in Southern California.
It was pretty common to have crews tied up waiting hours at emergency rooms even in normal circumstances.
Sample numbers from Central California : https://www.google.com/url?sa=t&source=web&rct=j&url=https://emsaac.org/%3Foption%3Dcom_fileman%26view%3Dfile%26routed%3D1%26name%3DJohn%20Surface%20-%20EMSAAC%202019%20Surface%204-23-19.pdf%26folder%3DLEMSA/Conference%26container%3Dfileman-files&ved=2ahUKEwiH85mTyIvuAhWiCjQIHYZnDhY4ChAWMAd6BAgEEAE&usg=AOvVaw1RolpERTpzHHNVMq1_abxc
comment by alexlyzhov · 2021-01-07T23:08:28.601Z · LW(p) · GW(p)
Suppose some variant like the SA one is vaccine-evading and some people will have to vaccinate a second time with an adapted vaccine. What are our priors for the safety of vaccinating repeatedly this way (either with the same or different delivery methods)? If we have two vaccines that are pretty safe, are side effects of vaccinating with the first one and then vaccinating with the second, similar one almost surely on the order of side effects from using just one kind of vaccine?
Replies from: magfrumpcomment by agc · 2021-01-13T18:13:08.178Z · LW(p) · GW(p)
I'm looking forward to tomorrows edition. Especially:
- UK cases have flattened out, although at a high daily level. The "control system" is very powerful.
- New York seems to be doing ok in vaccinations relative to other states, despite Cuomo's ideas.
comment by frankybegs · 2021-01-13T04:38:19.918Z · LW(p) · GW(p)
Quick question about the NBA snippet- are you saying that someone who has had COVID is certain to be immune at this point? Even from being able to spread it? Or just those confirmed to have antibodies? Or did I misunderstand that segment?
I ask primarily because I've had COVID myself, and have been considering myself likely immune from illness arising from reinfection, but not necessarily from passing the virus on. There don't seem to be many people willing to venture a confident opinion on this, but your implication seems to be that it'd be ridiculous to think that I am able to spread it. Am I misinterpreting you, or is there evidence I'm not aware of?
comment by countingtoten · 2021-01-11T03:01:30.544Z · LW(p) · GW(p)
And you also want, in that last tweet, to put (at least some of) the burden on these random institutions to then allocate the vaccine based on who has suffered disproportionately? While also obeying all the official restrictions or else, and also when did that become a priority?
You know that we decide which groups are at risk largely by looking at how they've died or suffered so far. Presumably she's hoping we protect people who otherwise seem likely to die, since her remarks seem sensible given her premises.
comment by TheSimplestExplanation · 2021-01-08T14:41:40.806Z · LW(p) · GW(p)
Because I’ve certainly learned my lesson and I’m not at all bitter about it or saying I Told You So over and over again in great detail:
What was that lesson?
AstraZeneca has vowed not to make a profit on their vaccine ‘until the pandemic is over.’ They have also declared the right to declare the pandemic ‘over’ in July 2021. So due to the fear that someone, somewhere, might be earning a profit, a major corporation makes money if they sell doses after July 2021, but not if they sell them before July 2021. I wonder what they will do. (Original Hat Tip)
Maybe what they mean is that until then it goes toward paying for the development or other fixed costs, so it still could work out. At least i hope it's that way.
Replies from: Kennycomment by philip_b (crabman) · 2021-01-08T06:22:34.175Z · LW(p) · GW(p)
Yesterday I've got the first does of Sputnik V, yay! And will get the second does in 21 days. Now, what do I need to know? How does my probability of getting infected change? How does the expected harm if I get infected change? Will I still be able to be a carrier and infect others without having symptoms myself?
comment by PatrickDFarley · 2021-01-09T15:33:58.282Z · LW(p) · GW(p)
Sabotage the freezers 👀