Covid 1/6/22: The Blip
post by Zvi · 2022-01-06T18:30:00.964Z · LW · GW · 21 commentsContents
Executive Summary The Numbers Predictions Deaths Cases Vaccinations Vaccine Mandates Djokovic Paxlovid Ministry of Truth NPIs Including Mask and Testing Mandates Think of the Children Zeynep’s First Law CDC Guidelines Revision Part 3 What, Me Worry? Hospitals Long Covid In Other News Not Covid Moderation in All Things None 21 comments
Cases are hitting record highs around the world. That’s going to continue for another few weeks. While it does, and for a bit after it stops, there are disruptions all around as too many people are sick at one time. Thus, the CDC guideline adjustments, the hospitals under pressure, many schools forced to not meet in person (and then deciding to torture kids with ‘remote learning’ rather than giving them a vacation.)
No question it’s annoying, and for those in health care it’s overwhelming and terrible. I don’t want to minimize it. And if you care about avoiding this it’s going to be a lonely few months.
But compared to March 2020, this is nothing. We got this.
There are dissenting voices, but mostly the consensus seems to be growing that Omicron is milder, the center will hold, and our lives beckon.
Executive Summary
- Record high case numbers likely to continue for a few weeks.
- Hospitals under pressure but holding, deaths strangely low.
- If you get sick you should still do your best to get a negative test before ending your isolation no matter what the CDC says.
Let’s run the numbers.
The Numbers
Predictions
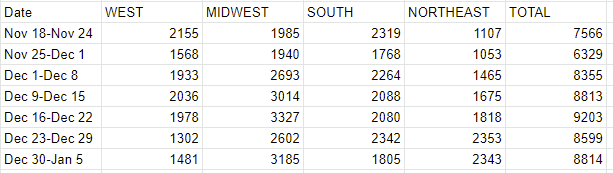
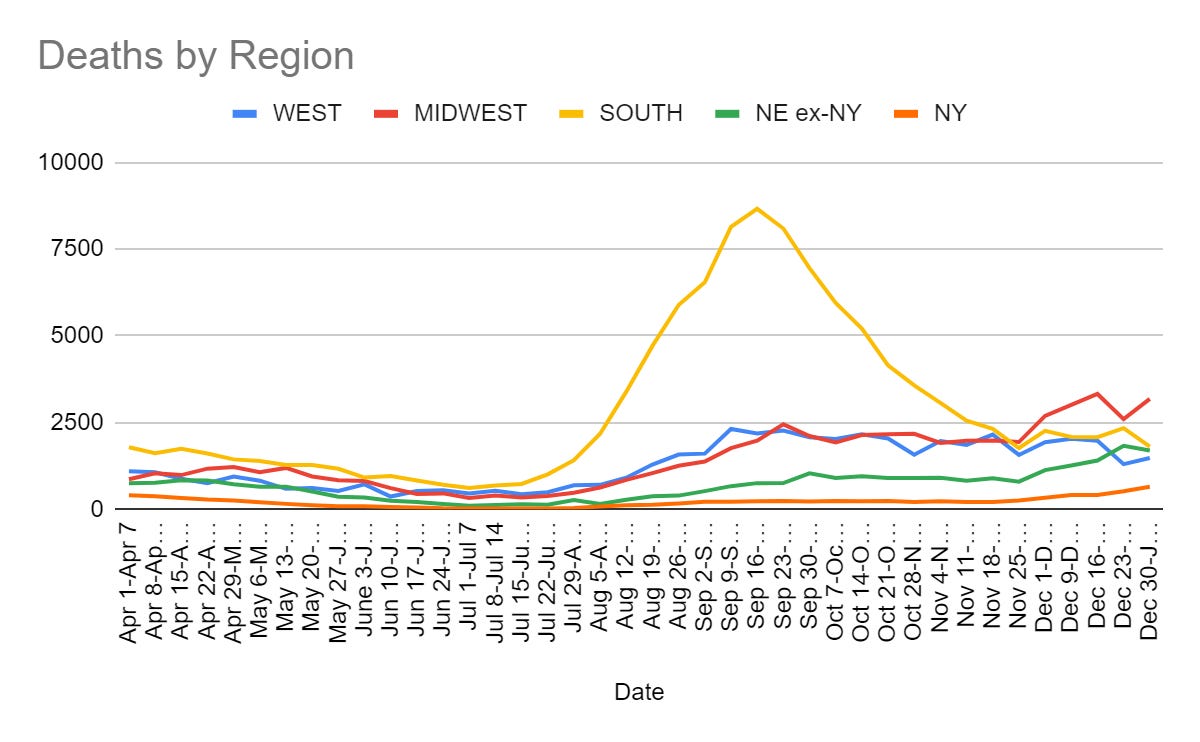
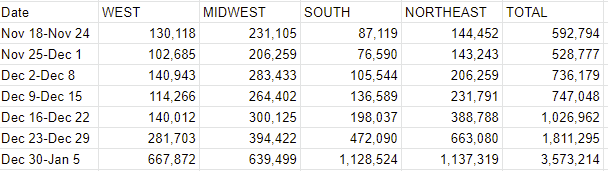
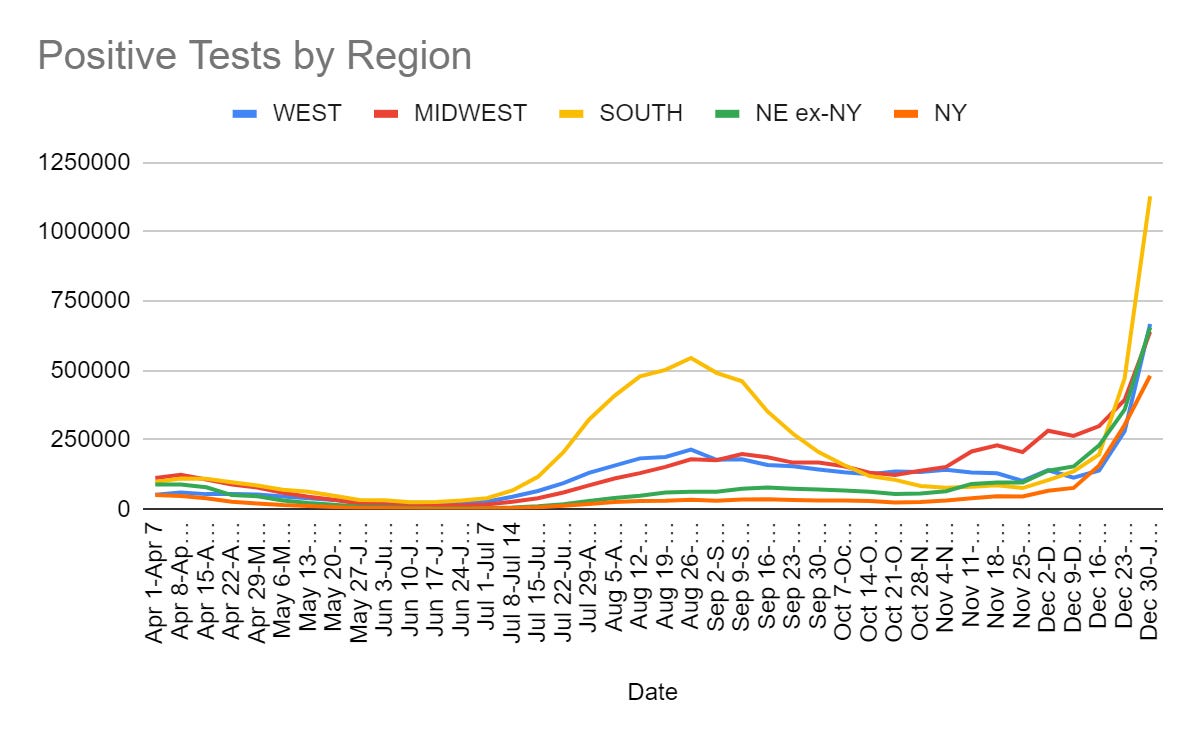
Prediction from last week: 3.5mm cases (+94%) and 10,800 deaths (+25%).
Results: 3.57mm cases (+96%) and 8,814 deaths (+2%).
Prediction for next week: 6mm cases (+71%) and 9,700 deaths (+10%).
On cases that’s another random bullseye. On deaths it’s a big miss, and given how little of the past cases were Omicron I don’t understand how the number came in this low, still below the level 2-3 weeks ago despite much higher case counts.
This is the dog that did not bark. The number damn well should have gone up a bunch, and it didn’t, and it makes me think that Omicron took over faster than I previously thought. I can’t think of another way to explain it, and the fact that I’m using that to explain it seems like very good news going forward.
I do expect deaths to start climbing, how could they not, but we keep not seeing big jumps there, so I’m going to downshift my expectations there even as lagged cases start rising faster.
Deaths
Report that deaths among young people are up 40% from pre-pandemic levels, in the context of life insurance. This sounds terrible and is terrible, but in terms of how one should live one’s life young people are still very unlikely to die and shouldn’t take minimizing death risk as a major life task except when considering doing actively risky things like skydiving, or putting oneself at risk of violence.
Cases
It looks like Manhattan has indeed peaked, and maybe Brooklyn, and maybe NYC overall. If that’s right, then things will have held together well.
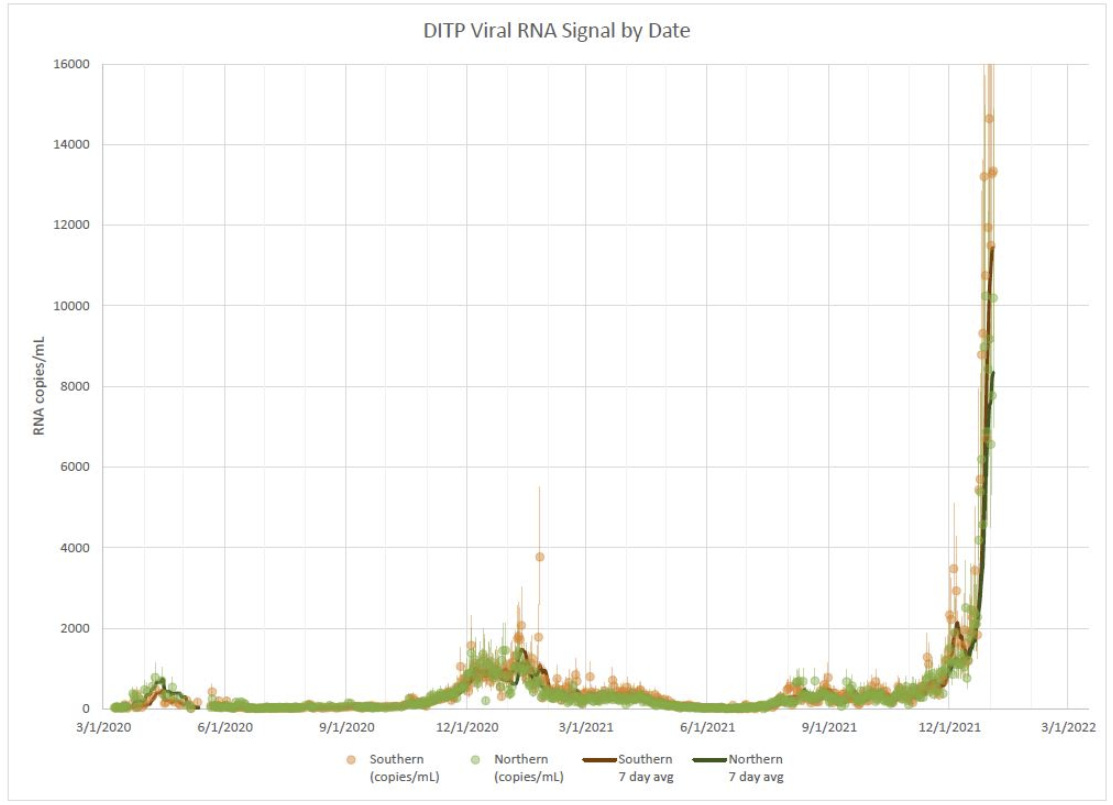
Boston on the other hand looks like it’s still headed upwards, currently at more than five times the previous peak.
Washington D.C. schools did systematic tests, found 5.8% of the tests came back positive. This was a lot of kids, so probably a lower rate than the city overall.
A week ago fully one third of NBA refs were in Covid protocols.
Vaccinations
CDC shortens length of time to wait for a Pfizer booster to five months. Six months was, of course, yet another arbitrary round number. And now we have this handy easy, not confusing chart, note that in some places boosters are mandatory soon after they are permitted.

The FDA decision to do thid bypassed VRBPAC. They didn’t consult their advisory committee. This new thing where when we don’t need their input we don’t ask for it? Excellent.
ACIP, alas, could not as easily be avoided, here is a recap of that.
Which includes this unrelated gem:

So, anyway, yeah, now you’re worried about boosters limiting vaccine supplies for other countries? What changed, exactly?
Also, it’s one thing that we haven’t approved Novavax, we have plenty of supply ourselves so we don’t need it. It’s another thing that we haven’t approved the manufacturing of Novavax?
It is still unclear how many doses Novavax will be able to provide next year. A company spokesperson said its goal is to produce 2 billion doses in 2022. But there are lingering concerns among top Biden officials and global health advocates about Novavax’s manufacturing facilities in the U.S. and Europe and whether the company can present the data necessary to obtain the regulatory approvals necessary to distribute doses made at those locations any time soon, according to the individual with direct knowledge of the administration’s thinking on Novavax and another individual with direct knowledge of the company’s communications with the administration. Both sources requested to remain anonymous to speak more freely on the matter.
I don’t know what to say to that, at this point. The boosters, over the long run, increase demand and will result in matching capacity and supply. It’s our delaying and denying of the booster plan that made this a problem at all. Meanwhile, we continue to hold up production rather than working to expand it. If we wanted more vaccine doses, we would pay for them and allow them to be created. We didn’t, so presumably we don’t want this very much.
Vaccine Mandates
That’s the strategy. The strategy is to punish the people who won’t follow his orders. To piss them off. And continue doing so, until the end. This isn’t about precautions that make physical sense. This is about punishment and coercion, full stop. There’s no longer any pretenses otherwise, on any level.
The alternative strategy that he needs to explicitly say he won’t do is to vaccinate the non-compliant population by force, or imprison them.
That doesn’t mean that there’s no benefits in terms of prevention or slowing the spread, but he’s no longer pretending that they are driving the decision.
And again, I appreciate the honesty here. It’s important not to punish such honesty, while still opposing the policy if you don’t think that we should be strong-arming people into getting vaccinated.
Similarly, if you were to punish the unvaccinated by banning them from buying marijuana and hard liquor, you are once again owning your motives.

Italy isn’t messing around either, but seeks to maintain plausible plausible deniability.
Djokovic
In other news, nope, no idea, I got nothing he could possibly do.
Yes, obviously he could have gotten the vaccine anyway to avoid such issues. It seems quite foolish not to do so, given the amount of travel he does, and I continue to not see this as a big deal.
Except here’s the thing. He did go through the required process (WaPo via MR).
According to a person close to the tournament with direct knowledge of the sequence of events, Djokovic followed every step of the country’s visa process properly. Moreover, the person said, Djokovic’s medical exemption was granted with all identifying information redacted, ruling out the possibility of favoritism.
Djokovic has had Covid-19. I believe he’s had it twice. One could respond with ‘that’s why you need a vaccine mandate’ but now that both infections are in the past, there’s no physical-world-model justification for denying him entry into Australia beyond the need to enforce the law. If this is additionally them about-facing and disobeying the law, it makes no sense in any way other than grandstanding and the punishment of someone that power doesn’t like.
Letting him get on a plane with one understanding (assuming his understanding was reasonable) and then turning around and doing this is another level. Some would say the cruelty is the point.
The argument in favor of keeping him out is that there’s no systematic way to verify who has previous Covid infections, and we don’t want to make an exception in this weird case where we can be confident the infections happened, or it wouldn’t be fair. There aren’t enough cupcakes for the whole class, so we throw away all the cupcakes. Or, of course, that you don’t like him.
Paxlovid
In order to get Paxlovid in New York, you need to have mild to moderate systems, be able to start treatment within five days of symptom onset, be over the age of 12 and weigh at least 40kg, and have one additional risk condition. I’d have preferred a much higher age minimum, but otherwise that seems sensible.
Then the question that seems to have no good answer. Give it to the vaccinated, or give it to the unvaccinated?
The solution is, whistle in the dark and count race as a ‘risk factor’?
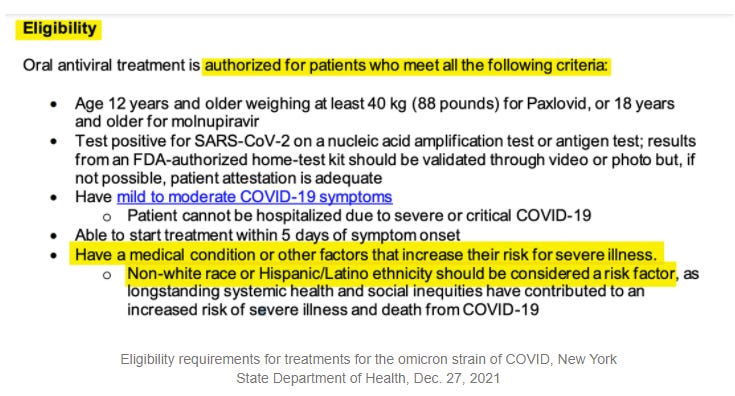
I can confirm, these are guidelines that were sent out.
I can also confirm that there were no other explanations given on what does or does not count as a risk factor.
Given the options of giving to each according to their needs or judging by the content of their character, they took at third option and went with the color of one’s skin.
This seems to be the CDC’s explanation:
Long-standing systemic health and social inequities have put various groups of people at increased risk of getting sick and dying from COVID-19, including many people from certain racial and ethnic minority groups and people with disabilities.
Studies have shown people from racial and ethnic minority groups are also dying from COVID-19 at younger ages. People in minority groups are often younger when they develop chronic medical conditions and may be more likely to have more than one condition.
They’re also less likely to be vaccinated. Policies that discriminate on the basis of vaccination status, that many on the left support and that many cities have implemented, have a disparate impact on the basis of race.
It’s important not to make too much out of this. If you have no ‘medical condition or other factor’ that increases your risk for severe disease, and presumably age counts as an ‘other factor,’ you’re not at much risk, and you shouldn’t be getting Paxlovid given our current shortage. If you actually need it, you’ll be eligible. Remember that when it was time to show eligibility for boosters, something like 75% of people technically had at least one ‘risk factor.’
Then again, if a bunch of people who don’t need Paxlovid get Paxlovid (including anyone who is white and who realizes how easy it still is to have a ‘risk factor’) then it’s a lot more likely there won’t be any Paxlovid to give you.
One could reasonably point out that given systemic differences in ability to navigate the system, and their reduced willingness to actually want a new anti-viral Pfizer drug, that those who are eligible via this rule will almost certainly be much less likely to get Paxlovid than similarly at-risk white people. The same would presumably be true if we instead made being poor or a lack of education a risk factor.
No matter what you think of such arguments, we are explicitly allocating scarce life saving medicine on the basis or race. This seems worth noticing.
The good news is that the White House doubled our Paxlovid order. The bad (non-news) is that they needed to do that in the first place.
Ministry of Truth
This was in accordance with Twitter’s ‘five strikes and you’re out’ policy. It’s not easy to get permanently suspended this way. You don’t quite get twelve chances to clean up before you’re asked to leave, but you certainly can’t say you were never warned.
Thus, she makes a good test case. What were the five strikes?
The first one seems to have been election-related rather than Covid-related, nothing you wouldn’t expect.
We were unable to locate the second violation.
My assistant did find this one, which we think (?) is the third one.
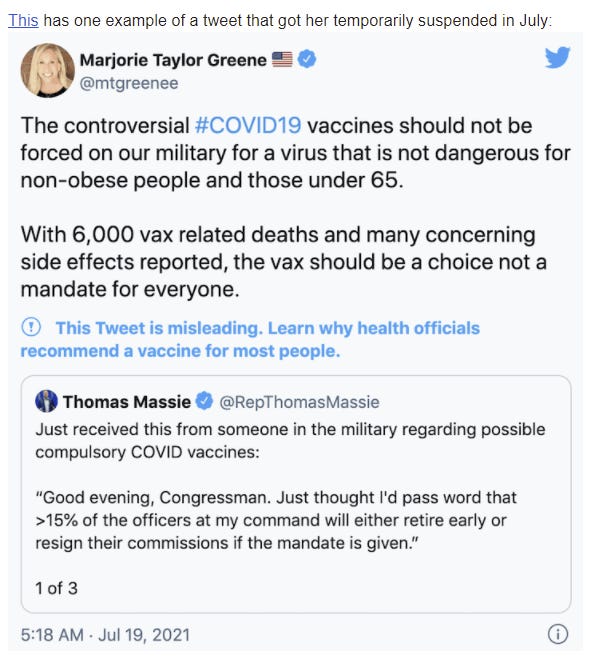
That does seem rather like ‘dangerous misinformation’ about Covid-19, on two distinct counts.
Yes, there’s a version of the ‘under 65 and non-obese’ claim that is true and important, but this is importantly different from that. I can see why one might find it unacceptable.
Then there’s the ‘vax related deaths’ claim, and yeah, stating that as fact does seem exactly like what a ‘dangerous misinformation’ policy is designed to stop.
There were also a lot of anti-vax things said that didn’t result in a strike, pretty much a constant stream of them.
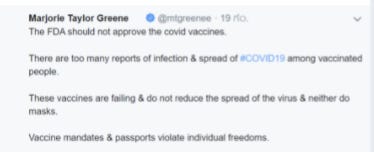
The fourth warning was likely this one, saying that vaccines do not ‘reduce the spread’ and neither do masks.
WaPo included this description of the final one, and it echoed that second claim from the third suspension, so there was very clear warning here.
The tweet at issue claimed coronavirus vaccine deaths were being “ignored,” citing the VAERS data. But the database itself warns that the information can be incomplete, inaccurate, coincidental or unverifiable, saying that the “reports alone cannot be used to determine if a vaccine caused or contributed to an adverse event or illness.”
That defense is quite the non-sequitur. It’s ‘misinformation’ to claim that things are being ignored in a database because that database says that its data might not be accurate or complete? That doesn’t sound like evidence against her position. Whenever I see such arguments used I update:
- There might not have been good arguments.
- Even if there were, they’re not going to be used to decide what to do next time.
- If we can use this kind of justification to label something ‘misinformation,’ then that word means whatever power wants it to mean.
- Thus, ‘dangerous misinformation’ is ‘information that power doesn’t like.’
I can’t even tell, from the description, whether her statement was even false.
I presume it was false, especially given the previous tweet, and that she was claiming a similarly massive number of (as far as I can tell, completely fictional) deaths from vaccinations. Which is misinformation, and is dangerous. I also think that censoring that kind of statement is a reasonable thing to consider doing. But the rules seem to consistently get written in a way that does not differentiate between this and a similar true or good faith statement, and instead give power the ability to censor whatever they dislike.
Over the long term, that policy does not go anywhere good. But it’s not like this should have come as a surprise.
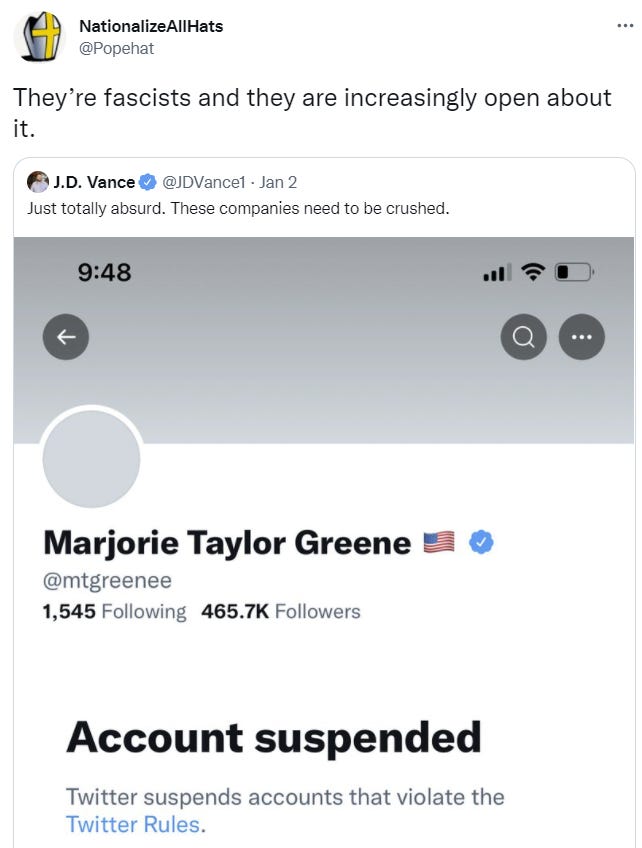
Reactions were as you’d expect. That first one sums up all sides quite well, I especially like the (intended or unintended) ambiguity here about who are or are not being fascists.
NPIs Including Mask and Testing Mandates
Interesting timing, but you know what they say, the second best time is right now.
Some fake KN95s got distributed over the weekend. The 95 means you stop 95% of particles, and by all reports these very much do not do that.
What they are still good for, of course, is fulfilling mask requirements. And presumably many people will prefer the feel of these, exactly because they fail to be an effective mask. Adverse selection is a real problem here, unless what you care about is the requirement.
NYC Testing cites for this week. Is there a reason this needs to be updated so frequently? Also clearly extremely incomplete.
It could be much worse, and some places it is, here’s an example of waiting a week for a PCR test. At which point, why bother?
Also, as a general principle, our procedures that decide which particular things to mandate or forbid (in terms of Covid-19 and NPIs, or anywhere else) is not well-principled, well-sorted or well-ordered, and often dumb rules are implemented instead of better rules.

If X and Y physically interact such that X relies on Y, it can make sense to only do X if you also do Y. To extent you have control over both the decision on X and the decision on Y, and Y strictly dominates X, then you shouldn’t do X without also doing Y. But the wisdom of our collective decision to do or not do X doesn’t much matter when deciding whether to do inferior independent option Y. You should do the prevention that makes sense on the margin, and not the prevention that doesn’t, in light of whatever decisions you’re forced into and the conditions that exist, even if those decisions were deeply stupid.
That extends beyond Covid-19. Arguments from consistency should mostly be ignored if you’re being forced to be consistent with decisions over which you have on control. Otherwise, once someone manages to sneak through one dumb decision, you’ll end up with a tsunami of additional dumb decisions. There’s always a dumb decision, in all directions, somewhere.
Also:
Given we’ve waited this long, I might wait a few weeks to be sure the hospitals will hold up in rural areas, but mainly, yes, amen, and let private citizens make their own private decisions based on what’s right for them.
Think of the Children
Should we mandate boosters for young children? I mean, obviously no, we should not do that, it’s too late for it to make a difference, the cost-benefit is unclear given how safe kids already are after two (or one, or zero) shots, and the amount of backlash would be severe. Yet the first question for anything approved is always ‘should this be mandatory?’
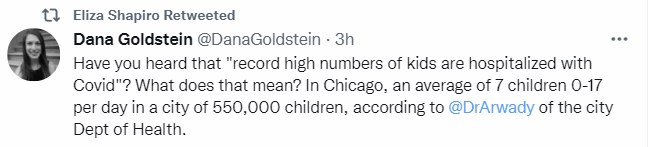
A reminder of what record numbers of child hospitalizations means.
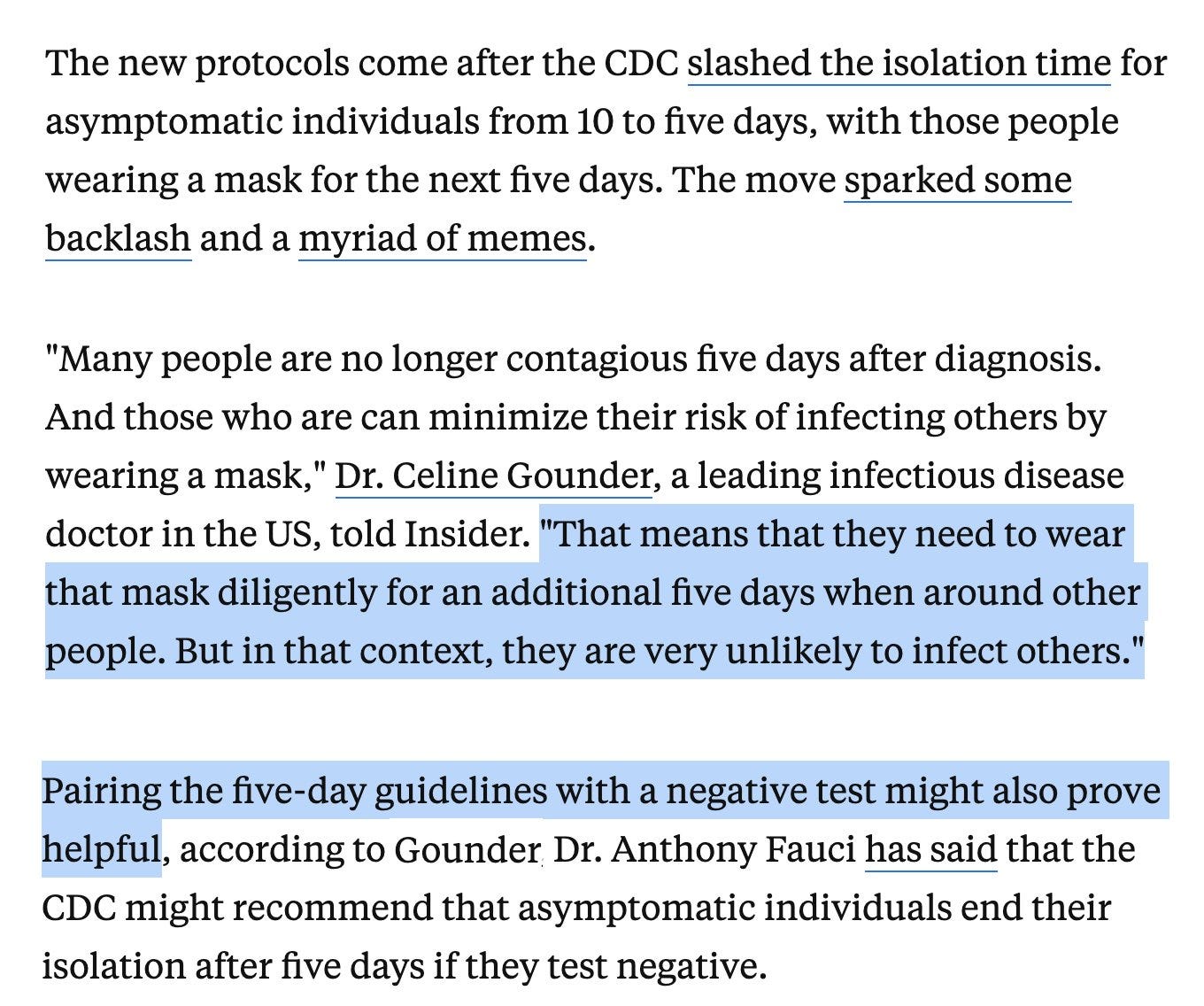
New York City schools instead are determined to stay open, so they’re asking teachers to come back five days after testing positive, without a negative test and despite mild Covid symptoms (article). If the symptoms are ‘improving’ then they don’t even have to be ‘mild.’


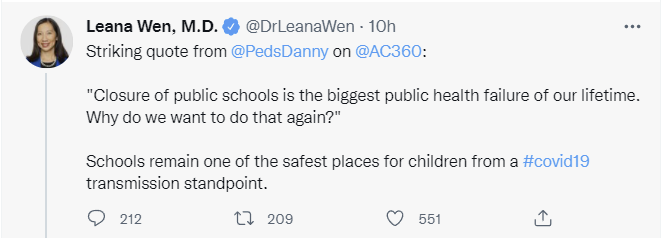
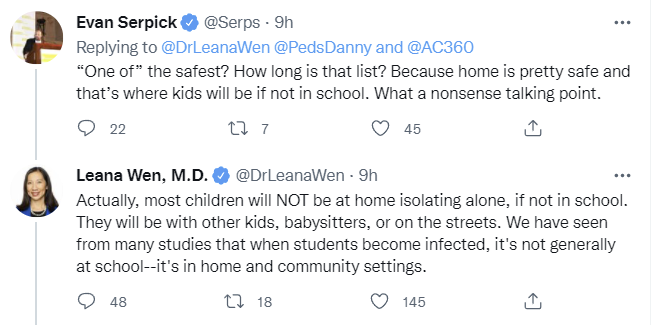
Did you know that schools are ‘one of the safest places’ for children during the pandemic?
And did you know that this is no way to grow up (article it links to is NY Times)? As in the NY Times itself is now pushing the narrative (because everything in that paper is pushing a narrative) that the disruptions we’ve imposed have put our children into crisis, And That’s Terrible, as opposed to before when it somehow wasn’t terrible and you were instead terrible for objecting to it.
So weird that suddenly, now, things other than case counts matter and it’s good to do a cost-benefit analysis about how much what you’re doing is messing up children’s lives. And all of this is suddenly ‘not surprising.’

My memory is same as Nate’s here, cost-benefit was anathema, also yes all of this was obvious but denied. I also worry how much emphasis was placed on suicides, both because it’s a lot of deaths and also because of the implication that the only way to rhetorically answer death is more death.
If you’re a parent whose children were forced into a year of ‘remote learning’ in the name of pandemic safety, you might be wondering, what changed all of a sudden? If schools are safer than not schools, in addition to the mental health and learning disasters that come from ‘remote learning’ as implemented by a vindictive system looking to mimic the punishments of ordinary schooling rather than teach children, then what the hell were we doing that whole time?
Meanwhile, schools are acting terrified in all sorts of different ways, which doesn’t seem necessary if they’re so safe. But also they’re indoors, often poorly ventilated, often with many people in the same room, so how in the world could they be ‘one of the safest’ places to be? What physical model could this be describing? Or is this describing something else entirely?
It’s no wonder some are feeling more than a little gaslit.
While we also scare the children. The message I want such a child to get is that getting Covid-19 is nothing for him to be afraid of, he’d be totally fine. I worry telling him to eat quickly sends the wrong message.

Also, crazy talk here, but what is so sacred about lunch? We’re taking kids, putting them in jackets and having them eat on the sidewalk, when we could simply… give them a bigger breakfast and then have them wait until they get home? Is that so completely insane? At about that age I remember being sent to a camp that served non-kosher food and my parents wouldn’t let me eat it and I was the kind of kid who followed such rules, so I often ended up eating once a day, and this wasn’t only fine, it taught me a useful life skill, that I use almost every day.
So you know what, how about let’s not do lunch.
I do realize it’s different for those who need subsidized school lunches, because our society is pretty terrible about how it gets its children in need fed.
The only good counterarguments to all this that I’ve seen are:
- Schools as they typically exist are terrible.
- Whether or not schools are terrible, kids can and do recover from missing even quite a lot of school, all the time.
If you think typical schools are dystopian nightmares, you’d be inclined to welcome a break from them. The thing is, even if schools are such nightmares, remote learning as implemented by the United States was clearly much worse. It carefully recreated all the negative aspects of school such as being constantly forced to sit motionless all day as a dominance exercise, and adds new ways and new levels, while failing to capture the benefits of school, such as social contact with other humans, or making any attempt to teach things.
This is not the kind of thing that old ‘missing school’ studies were measuring:
I’ve seen some of this as well, although thankfully less.
My model is:
- If kids got to stay home, use Khan Academy, play games, read books and listen to the radio, play outside with the other kids and otherwise be the age they are, help around the house and learn practical stuff and from their parents and others around them, that would be like ‘missing a lot of school’ – if the alternative was be allowed to be a child – then the kids would very much be all right.
- If the kids are forced into ‘remote learning’ then you’re torturing them all day while both failing to teach them much of anything other than how screwed up everything is, and also crowding out opportunity and energy for either living life or otherwise being able to learn. You’re also combining that with not letting them see other children or other people’s faces. Meanwhile, we’re teaching all our kids to be obsessed with the ‘danger’ of catching Covid-19, as something central to life.
- Yes, this is going to turn out very badly.
- There’s a reason I home schooled our kids rather than doing remote learning.
Matching all this is the suicide data.

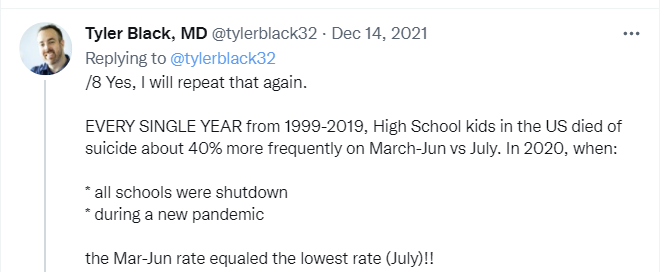
Normally when kids are in school, they are more likely to kill themselves. This year, when we closed the schools, kids killed themselves less. Then, when we went to ‘remote learning’ kids killed themselves more.
From the anecdotal experiences I’ve hard about, and I mean all of them, it’s not hard to see why.
In a related question, is this schools having a problem or is school a solution?
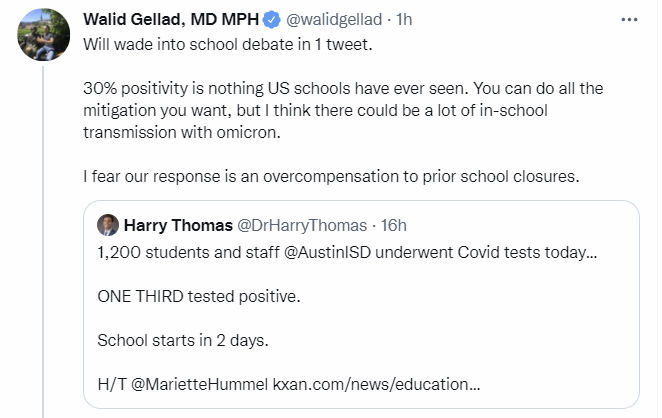
Does this mean the schools are dangerously unsafe and have to close, because a third of students are positive? Or does it mean that not being in school is dangerously unsafe, and the schools need to (or might as well) stay open?
Should you close the schools? Should you close to schools to everyone who tests positive? Or should you close the schools to everyone who tests negative?
If you put the two thirds of students who you don’t think have Covid-19 into a classroom, you’re going to be wrong, because on average you’ll have one student who got infected yesterday and one from two days ago. So everyone gets exposed anyway.
Whereas if you put the one third of students who definitely do have Covid-19, since the false negative rate is super low, into a classroom, then everyone already has it, and no one gets exposed. Of course, you’d then need to ensure the teachers also have it, but that presumably a lot of them do as well, and they’re not exactly otherwise in high demand, so sure, why not?
The best part of this plan is that over time it improves. Everyone who has had Covid-19 in the last few months is also fine, so pretty soon the classroom is full again. Then, once things settle down, the kids who were always negative can come back.
Fun little exercise. There’s so much room to actually improve things if we cared mostly about outcomes and not what things looked like, as many good reasons as there are that this absolutely does not work. So just kidding, baby. Unless you gonna do it.
Yet another standard ‘colleges are imposing crazy requirements’ post, this one a guest post on the Bari Weiss substack. Pre-Omicron, such posts were transparently correct, the universities were doing Obvious Nonsense. In March, any remaining such policies will once again be Obvious Nonsense.
And also, right now, such policies are still Obvious Nonsense, because they are neither necessary to protect anyone nor are they sufficient to stop spread on campus. If you don’t want your students infected in January, you have zero options. You do have the option to ensure they are not infected on campus by not opening the campus, in which case the infections will not be your fault, but the infections will still happen.
When there are 146 positives upon return to campus like there were at Stanford that’s not on you. That presumably is what such policies are about.
Having been soundly trounced by Georgia, the University of Michigan goes from daily to weekly testing, buying up to six days of the school being open. This makes the data much less useful for making good decisions, but potentially less useful for making bad decisions as well. Value of information can sometimes be negative.
And that’s why Yale students are under quarantine until February 7 and not allowed to eat at outdoor restaurants.
Zeynep’s First Law

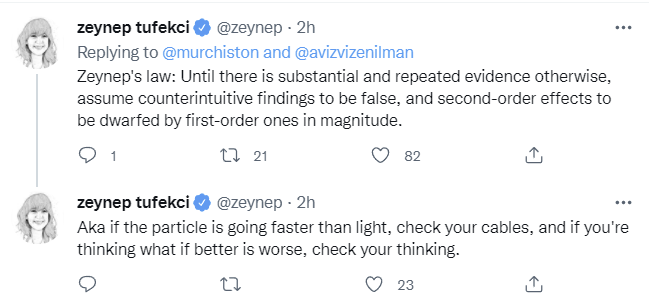
What, never? Well, hardly ever. And not by default.
I think she may have dropped not one but two, as the next section will show.
CDC Guidelines Revision Part 3

Bob Wachter suggests CDC should have told the truth about why it was issuing its guidelines, and isn’t even suggesting the whole truth. He’s suggesting merely that they not lie about tests not working on day five, not the crazy talk of admitting that they’re compromising a bit to keep society running.
This or something similar seems like what all the reasonable people are suggesting makes sense, it’s simple, it’s being done elsewhere, it makes perfect sense.
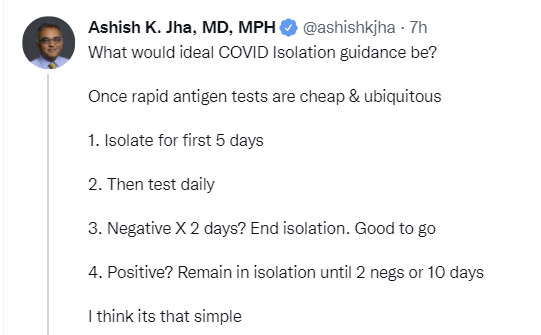
I am not sure we can afford to wait for the second negative test, nor do I have a good idea how much extra value that second test provides, but even one would be a large improvement when it’s available.
And this keeps it simple, as opposed to attempts to explain current policy.
We also have The Daily Show explaining in video form (~1min).
Cause yeah, this isn’t simple at least as written (link to policy).
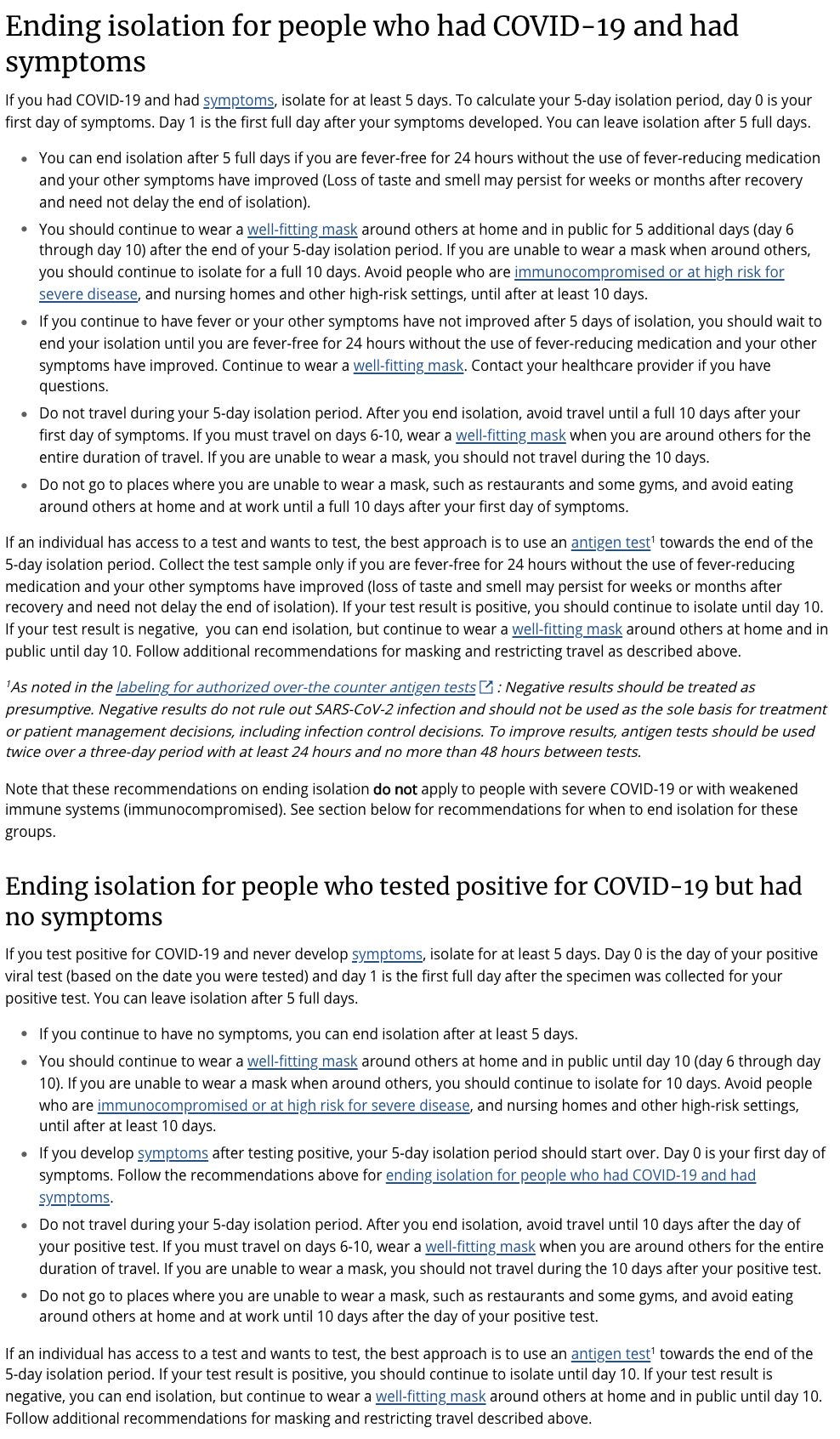
That’s a lot of words that effectively say ‘isolate for 5 days, then mask for 5, and if you have an actively positive test after 5 days, then isolate for the full 10 days.’
It’s a sign both of the CDC’s inability to cleanly communicate, and the amount of trust they’ve lost, that everyone is calling this complicated, and calling for ‘simpler’ things that are more complicated than what this is trying to do.
Meanwhile, the CDC’s own guidelines say that 31% of people are still infectious on day 5.
It’s also worth noting that if you’re exposed to Covid-19, you’re asked to isolate about as much as if you test positive, if anything longer because they have you test afterwards since who knows when you might or might not have gotten infected. So it’s ‘better’ to actually be positive than be ‘exposed’, even though basically everyone not working hard to avoid exposure is exposed.
Or consider their planned new policy.

There’s also always the incentives.
Of course, no one knows what the rapid test said, so if you choose not to look it doesn’t actually get you off of any real hooks. It’s Not the Incentives, It’s You.
As an example of how this works in practice, what you’re supposed to do if you test positive in the DC area.
Anyone else want to give it a shot? How about the CDC director?


That might want to be her second law, e.g.:
Zeynep’s Second Law: Extra information doesn’t automatically turn responsible people into irresponsible ones.
California moves to 5 days and adds the obvious testing requirement.
Tom Frieden actually explains and defends the CDC’s actual policy, considers it reasonable because tests aren’t always accurate. This doesn’t seem like a good argument, but the implicit ‘we must muddle through as best we can’ carries weight.
What, Me Worry?
In today’s no s*** sherlock headline news:

I mean, I knew that, and I’m still willing to bet this one doesn’t replicate, because, I mean, they’re doing stuff like this, and that stuff is meaningless and doesn’t replicate, it’s the law.
For the tests examining how well people maintain information, participants had to match pairs of numbers and symbols according to a specific set of rules. Study authors also examined the group’s decision-making skills using a test of risk management. Each person could either choose a “certain” option where they definitely won $75, or a “risky” option where the odds of winning $0 were only 25 percent and the odds of winning $100 were 75 percent.
Those are two options each with an expected value of $75, so I have no idea what decision making they plan to test there?
The team also discovered that worrying about COVID-related issues distorted a person’s ability to evaluate certain risks. They underestimated the chances of likely outcomes occurring (like winning $100) and overestimated the chances of unlikely possibilities occurring (like winning nothing at all). The team believes this impact on decision-making abilities may influence some people when they’re considering certain topics — like getting the COVID-19 vaccine.
I can certainly believe (but also could almost as easily disbelieve, or believe the opposite) that people who worry a lot about Covid-19 also obsess over other small ‘risks’ but what does it mean to ‘underestimate the likelihood’ of something in this context? I tried to actually skim the paper, to no avail, leaving even more confused.
Which is a great joke, but also what he’s saying is that one can’t plan one’s life around constant testing. I very much agree. Testing is important but there are those who have gone completely overboard. ‘
In related news, a study finds getting vaccinated is good for mental health, reducing symptoms of depression and anxiety by 30%.
Hospitals
A lot of health care workers are sick, but that’s not the only reason staffing is short.
The health care quit rate has risen to 3% per month. It’s an impossible job that’s only getting harder.
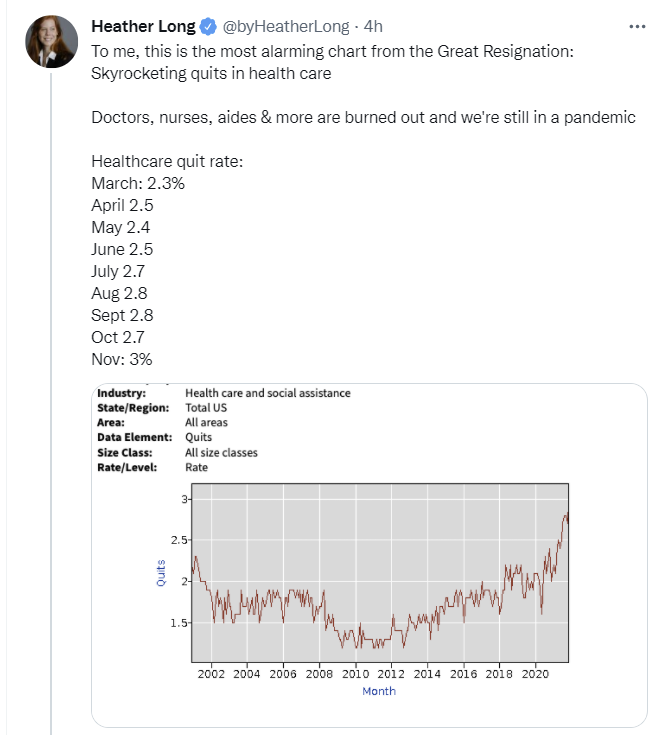
(Quits are high in other areas as well, some data at the link.)
Rhode Island hospital is at 113% capacity, but only at 65% of what capacity would be with normal staffing, which means almost half of capacity there is currently offline. It also means that you can be at 113% of temporary capacity.
Hobson’s latest update on the state of UK hospitals. London looks like it will hold, but serious worries that other areas will fail to echo London and things could get worse, especially as more elderly get sick. And even if ‘the hospitals hold’ that doesn’t mean conditions are good. Waits are still often 12+ hours long, everyone is stretched beyond their limits.
Here’s some interesting data, and wait did you know the ‘for Covid’ share of the patient population this whole time?


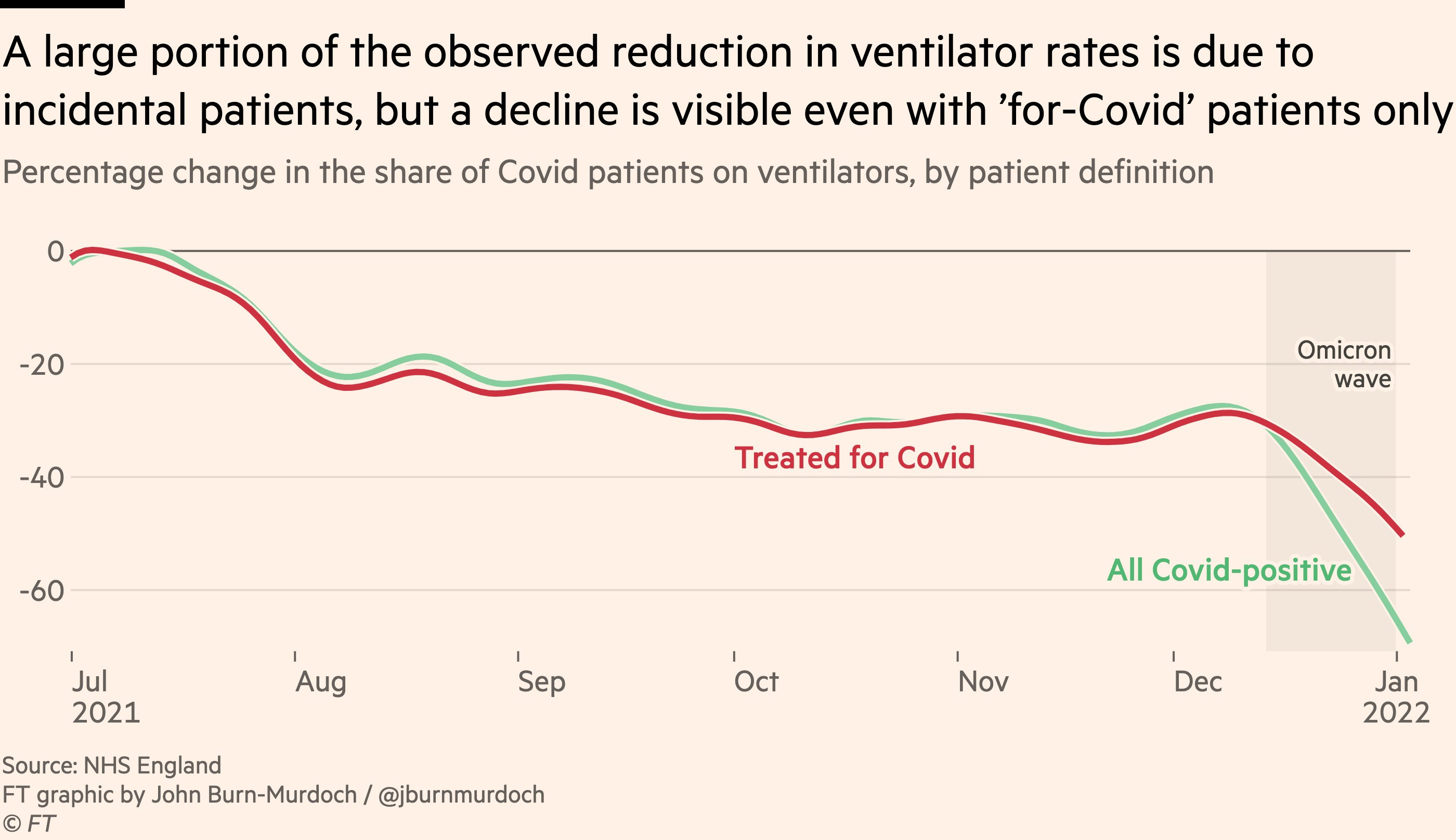
Right now, something like 15.5% of ‘for-Covid’ patients are ventilated, whereas 7.5% of ‘with-Covid’ patients are ventilated, so something like ~45% of all patients that are ‘with-Covid’ are also ‘for-Covid.’ Looking back at the start of the graph, we see 20% ventilated versus 28%, so that implies ~70% of all patients were ‘for-Covid.’ That’s a big drop.
It would be good to compare the number hospitalized ‘with-Covid’ with the number you’d expect from the baseline population, but we don’t have the baseline number, so we can’t do that analysis, unless there’s data sources I don’t know about.
On top of that, even the ‘for-Covid’ patients are being ventilated substantially less, about -50% from July 2021, versus about -30% at the start of the Omicron wave, so an additional -25% from there.
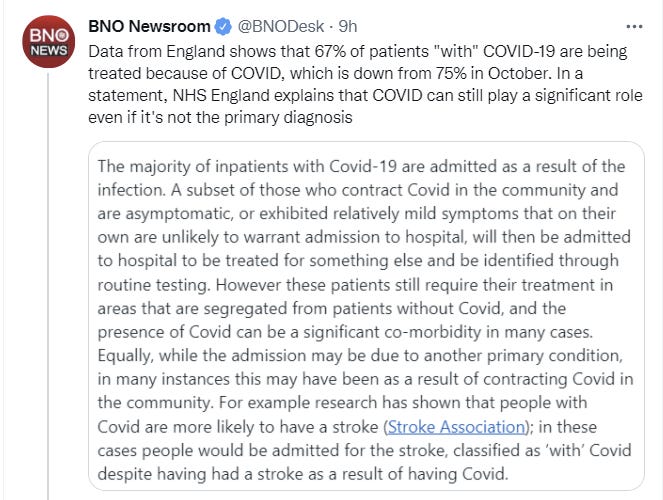
Eyeballing the graph has the number going from 70% to 45%, the stat here says 75% to 67%. The 70% vs. 75% is a rounding error in context, but the 45% vs. 67% is bigger, there’s no way to reconcile that with the graph above.
All such graphs need to be adjusted for the relative ages of the populations, to get the full context, as my understanding is that the Omicron wave still skews relatively young, so that’s another way in which it’s still going to get worse before it get better.
Also this data point: Los Angeles hospitals are two thirds ‘with Covid’ versus one third ‘for Covid.’
In terms of that, nursing homes are only now seeing the kinds of staff shortages and rates of illness that lead to more cases. To extent that things look good at first and then get worse when it seems like they should be getting better, this dynamic and similar things like it are the most likely reason.
Long Covid
An all time great headline.
Claiming to have Covid-19 was correlated with claiming to have Long Covid.
Actually having Covid-19 was not correlated with anything other than anosmia.
Restricting the analyses to participants with a positive belief and attributing their persistent symptoms to COVID-19 showed a positive serology test result to be associated only with anosmia (OR, 2.97; 95% CI, 1.58-5.57) (eTable 7 in Supplement 1). Similarly, confirmation of the diagnosis by a laboratory test or by a physician (vs the response, “No, but I think I had it,” and excluding participants who answered “I don’t know”) was also associated only with anosmia (OR, 4.29; 95% CI, 1.92-9.58) (eTable 7 in Supplement 1).
Their conclusion is polite but brutal:
The results of this cross-sectional analysis of a large, population-based French cohort suggest that physical symptoms persisting 10 to 12 months after the COVID-19 pandemic first wave may be associated more with the belief in having experienced COVID-19 infection than with actually being infected with the SARS-CoV-2 virus. Although our study cannot determine the direction of the association between belief and symptoms, our results suggest that further research regarding persistent physical symptoms after COVID-19 infection should also consider mechanisms that may not be specific to the SARS-CoV-2 virus. From a clinical perspective, patients in this situation should be offered a medical evaluation to prevent their symptoms being erroneously attributed to COVID-19 infection and to identify cognitive and behavioral mechanisms that may be targeted to relieve the symptoms.
I’m updating quite a bit in the direction of Long Covid mostly (not entirely) being people often having health issues, and them then blaming those health issues on having had Covid, rather than on Covid causing long term symptoms often in people who didn’t have severe disease. No question that those with severe disease often have lasting damage, but yeah, if you feel like it finally happened and was no big deal, it was almost certainly no big deal.
In Other News
Looking back, no one could have predicted that politicians and regulators would betray our trust, or that repeatedly betraying the public’s trust would destroy public trust.
Man begs for positive Covid test to avoid visiting relatives.
Scott Lincicome feeling pretty good about his radicalization regarding repeated government failure and obstruction. I am Bart Simpson’s chalkboard repeatedly writing “I will not suggest using the free market to supply things people want.”
I don’t know what this is about but seems potentially quite the red flag, and worth passing along.
The problem with the ‘with Covid’ versus ‘for Covid’ distinction is that Covid can also screw you up in other ways. So the ‘for Covid’ population isn’t the full story. In relative terms, the statistic still seems super useful.
Reminder, if you don’t have any symptoms, there’s no need to go to the emergency room or hospital, such people are clogging up the works in Vermont and everywhere else.
This thread is advice on what to do if someone is infected. Most of it seems reasonable (although not complete, she doesn’t mention Vitamin D, Zinc or Fluvoxamine). The part where she says to go out and get vaccinated after you’ve been exposed doesn’t make any sense to me other than as ‘one must recommend vaccination at all times no matter what’ but one can ignore that and look at the rest.
Pandemic or no pandemic, one man is still trying to find the answers to life’s persistent questions.
Scott Sumner looks back on what it was like two years ago, when the pandemic could potentially have been contained, but we didn’t know what we were dealing with. Since China did successfully contain it within China, it’s fair to think there’s a good chance that the same measures taken earlier would have contained it before it got elsewhere. How realistic that counterfactual is, and what that would take, is an important question going forwards. The necessary effort would not have been small or cheap. Do we have any good examples of containing something this hard to contain by acting early and aggressively on a (relatively) small scale?
A fully told story, in one Tweet.
For context, he was referring to this particular lie.

Not Covid
Or is it? Scott Alexander reviews Don’t Look Up (Spoilers).
My initial review of this movie was to note the cast looked amazing, and then say, and I quote, “I am not seeing this movie because I don’t have to and you can’t make me.”
I felt like I’d already seen the real world version and the movie would only bring pain, which more information has only confirmed. I do appreciate those involved for trying, and they’ve provided a baseline from which one can discuss important matters, but in the meantime every time I had the option to see or hear or read about this movie, my life got worse, until Scott’s review recapped it sufficiently painlessly that I now feel as if I’ve seen it on a different level than the one in which I’d ‘already seen it’ by default.
Scott’s review attacks the situation from an interesting angle, which is how to determine who to trust and what it means to Follow the Science without accidentally simply listening to power and thus Following the Science(TM) rather than making your beliefs match physical reality.
That’s been a lot of what this two-year project has been about here. At best, the official faces of Science(TM) has been behind, too slow to react to new information, only later doing somewhat reasonable things. At worst, they have outright lied to us about how the world works and given us orders that were Obvious Nonsense.
The only solution is Think For Yourself, Shmuck. There’s no easy set of rules to doing that, other than P(A | B) = P(B | A) * P(A) / P(B).
Not only is there No Royal Road to Wisdom, but even the poem No Royal Road to Wisdom, that often ends the Secular Solstice,is wrong about the road to wisdom. It reads:
The road to wisdom
Is easy to express
You err and err and err some more
but less and less and less
And no, that’s a beautiful poem and most people would be improved by taking it more to heart, but that’s wrong too, that’s the road the schools teach us. That’s ultimately the road to not thinking at all. That’s the road they want you to take. You don’t want to err less. You want to err on more interesting levels, in more advanced ways. You want to always be pushing at the level where you err at the right rate, or else you’re not learning much. Which is a subtle difference, but supremely important in the end.
One of the biggest problems with the Trusted Authorities is that if it’s very important that they never be seen as importantly wrong, it’s extremely difficult to ever be importantly right. You can only claim that which is certain, so you can only be unimportantly right. Or you can manipulate the narrative.
The Litany of Tarski [? · GW] is closer. Thus:
If a comet is coming to destroy the Earth, I desire to believe that a comet is coming to destroy the Earth.
If a comet is not coming to destroy the Earth, I desire to believe that a comet is not coming to destroy the Earth.
Let me not become attached to beliefs I may not want.
Some other time I should notice all the ways in which that last line is really weird.
I do my best to synthesize the information I get from a wide variety of sources, combine it into as coherent a physical world model as I can, and synthesize what it all likely means, while doing my best to think probabilistically. Then, you the reader can decide whether my reasoning makes sense, and whether my sources check out, and any other factors to consider. Thus you decide how much you want to rely on me in turn, the same way I am relying on others. It’s the best we’ve got.
I’d like to have something better to put here, but I don’t, and I don’t believe anyone else does either. Predictions are hard, especially about the future.
Also, a reminder that people don’t love science all that much and this isn’t new. They didn’t want to go to the moon, they were skeptical of the polio vaccine, they didn’t care about computers and all that.
And that if you think we’re serious about climate change, well, sometimes it’s not you, it’s the incentives, like when they tell you to fly empty airplanes thousands of times across Europe to maintain landing slots, and you still don’t have a carbon tax.
Moderation in All Things
Lastly, a note on moderation policy for both Substack and WordPress.
So far, I haven’t needed a real one, and have only deleted one post that wasn’t either a simple error correction or obvious spam, and the contents of my comments section especially on WordPress have mostly been high quality. Having to find the blog and decide to comment was filter enough.
However, recently I’ve gotten a lot of new readers, and a number of new frequent commenters, and I’m seeing a higher proportion of comments that make my life worse rather than better, and likely make other lives worse as well. In particular, I’ve also gotten a higher proportion of comments that are mostly advocacy and aggressive rhetoric rather than gears-level explorations, and often heavily political, which I’d prefer to avoid.
Please strive to post comments that make the world better rather than worse, and avoid comments that make my comments section look like every other content section on the internet.
Also, please be aware that you cannot edit your comments, so strive to get it right and to avoid having to put out 3-5 quick reactions in a row to the same thing.
Typical comment sections are full of rudeness both to the author and to others who comment. They also have a lot of ad hominem attacks, repeatedly make the same points without anything new to add, and are neither careful nor precise with claims that anyone who doesn’t know something or agree with you something is clueless or stupid or isn’t paying attention, or others that are similar. The rightness of one’s ingroup against the outgroup is often taken for granted.
That stuff’s not what my comments sections are for, and if the garden is becoming sufficiently ill-kept, I’m not going to let it die by pacifism [LW · GW].
The goal is to share models and information (including links) and improve our understanding of the world, and also of course to make life better through other methods such as jokes and social connections and all that.
For now, the new policy is that if a comment makes my life actively worse to a sufficient extent, I’ll say that explicitly (as in “This comment made my life worse”), and one can consider this a polite request to update on that information and stop it, but continue to have a very high bar for deletions or bans and hope we can still have nice things. If that doesn’t work, I’ll escalate.
21 comments
Comments sorted by top scores.
comment by Daniel S (daniel-s-1) · 2022-01-06T20:10:39.902Z · LW(p) · GW(p)
This comment is intended more as a small aside rather than a sweeping comment, but for me personally the signal:noise ratio on these posts has gotten somewhat lower recently - still a much higher ratio than most sources.
I have been a consistent reader and found them extremely valuable. What I find valuable generally are the "status update" portions that contextualize changing cases/deaths/etc, the "evidence rundown" portions that discuss emerging evidence (such as the Long Covid section of this post), the specific predictions, and to some extent discussion of changing policy circumstances.
I generally don't find the discussion of egregious examples of policy gone awry (eg Djokovic, fake KN95s, etc), or even broader discussions of policy framing (France, Think of the Children) to be as useful. When they are, it's usually because they're attached to a specific piece of data or information on significant policy changes, but lately they seem to have been variations on a similar theme (bad epistemology and/or excessive restrictions) that doesn't add much post over post.
It may be that you view the repetition as valuable insofar as it convinces people that there is an issue! Just thought I'd note that I tend to start skimming to sections I find more useful.
Replies from: bfinn, CraigMichael, Viliam↑ comment by bfinn · 2022-01-06T21:44:18.551Z · LW(p) · GW(p)
Personally I think the repetition is OK, not least because many people don't have time to read all the posts, nor in full (e.g. I don't); and I expect many new readers will only read one or two posts, and it's potentially useful that they see such egregious examples at least once, to get the gist.
↑ comment by CraigMichael · 2022-01-06T22:55:21.204Z · LW(p) · GW(p)
I’m still finding these very useful at their current frequency.
EDIT: I should add, much of what I’m getting here is learning to appreciate the way Zvi thinks and his Not Covid section this time around was pretty good.
The silver-lining of the pandemic for me is that my epistemic reasoning has improved substantially, and I have a renewed appreciation for good science communication.
This is a real word scenario where we all have skin in the game and decisions have consequences. It’s an island of learning opportunities in a sea of dystopian tragedy, yes. But I really enjoy the visits to the island a few days a week. It’s at least a break from treading water in the sea.
↑ comment by Viliam · 2022-01-07T18:05:04.287Z · LW(p) · GW(p)
egregious examples of policy gone awry (eg Djokovic
Also, some comments at MR suggest that the situation is more complicated. If I understand it correctly, there are things you need to do in order to enter the country, and things you need to do in order to participate in the tournament... and while he did the latter (by getting an exception, but anyway), he failed to do the former.
comment by Adam Zerner (adamzerner) · 2022-01-06T20:09:12.059Z · LW(p) · GW(p)
young people are still very unlikely to die and shouldn’t take minimizing death risk as a major life task except when considering doing actively risky things like skydiving, or putting oneself at risk of violence.
This is probably assuming that people have "normal" expected lifespans of something like 80-100 years. But if we take seriously [? · GW] ideas like the singularity and accelerating technological progress, perhaps [LW · GW] we should be expecting much longer lifespans, in which case minimizing death risk would be an important life task.
Replies from: countingtoten↑ comment by countingtoten · 2022-01-07T01:46:19.036Z · LW(p) · GW(p)
Yes. There's a reason why I would specifically tell young people not to refrain from action because they fear other students' reactions, but I emphatically wouldn't tell them to ignore fear or go against it in general.
comment by jefftk (jkaufman) · 2022-01-07T03:22:31.753Z · LW(p) · GW(p)
Boston on the other hand looks like it’s still headed upwards
It only looks that way because the graph is all-time, and so you can barely see what's happening. Here's the most recent data:
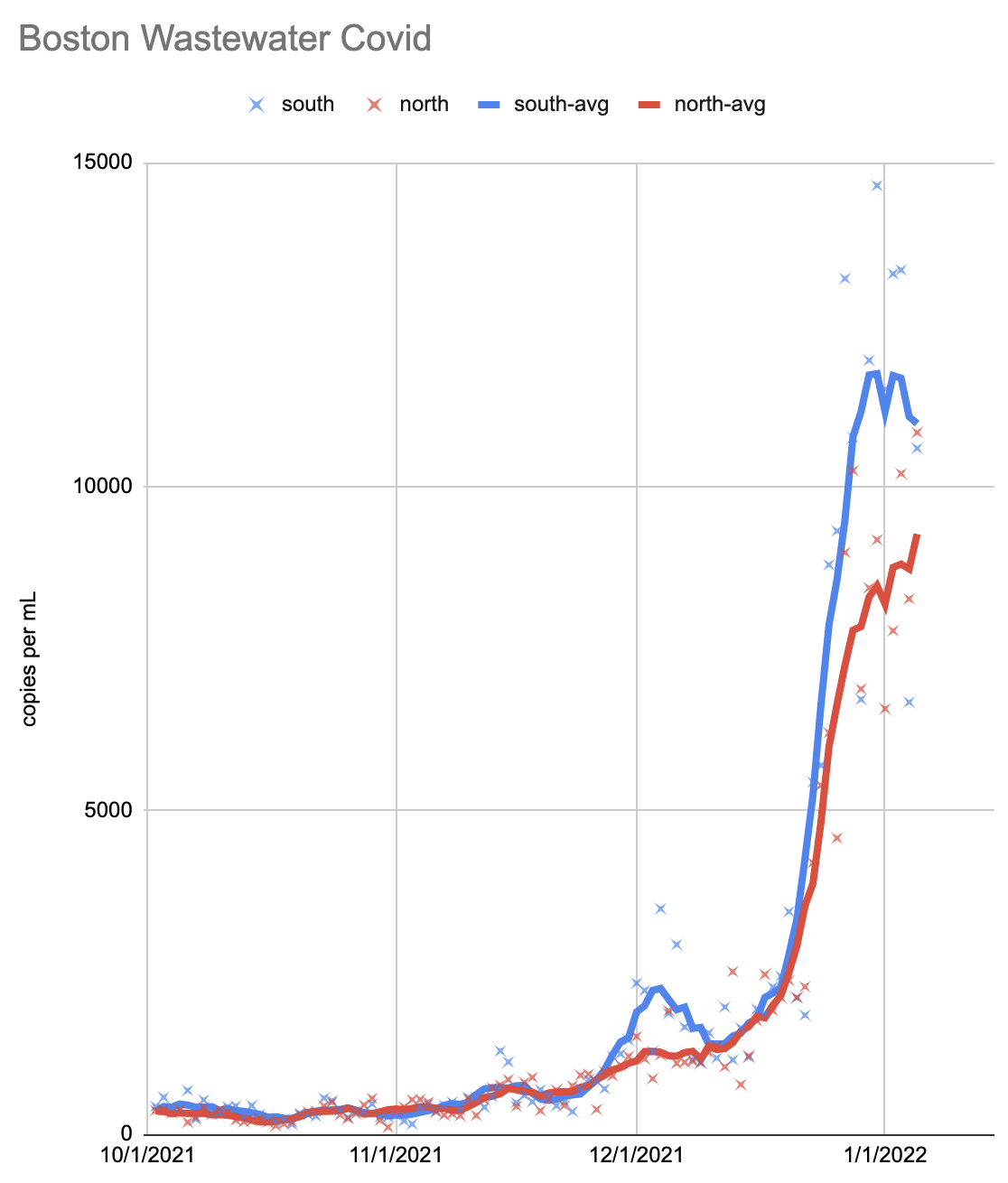
It looks like the southern half of the system has peaked, or at least plateaued, while the northern half is getting close.
comment by Owain_Evans · 2022-01-07T16:54:39.644Z · LW(p) · GW(p)
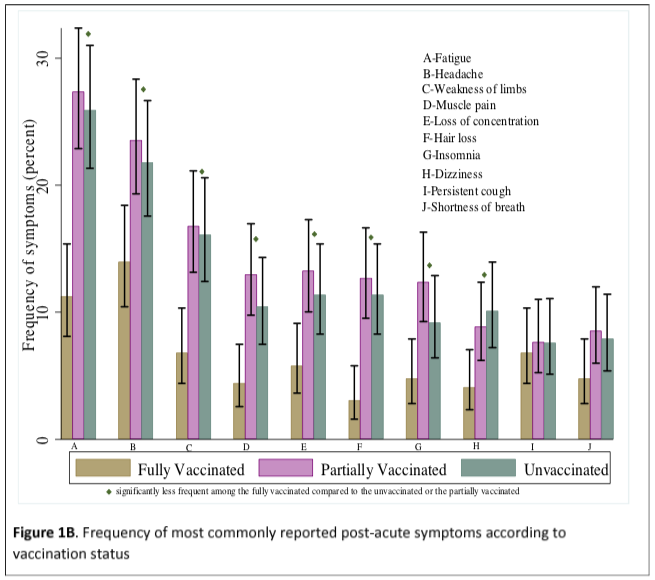
Interesting Long Covid study from Israel finds approximately 50% reduction in symptoms post-Covid for the fully vaccinated (vs. unvaccinated). The study is prospective. There's a selection effect for who got vaccinated but I doubt this is a big issue (unvaccinated are younger + healthier -- education levels not that different).
https://www.medrxiv.org/content/10.1101/2022.01.05.22268800v1
comment by TheMajor · 2022-01-06T23:58:21.907Z · LW(p) · GW(p)
I think the section on Don't Look Up, in particular the comments on the relationship between science and policy, misses the mark in very important ways. The naive model of [science discovers how the world works] --> [policymakers use this to make policy to improve the world (for themselves, or their constituents, or everybody, or whatever)] does not give enough weight to the reverse action - where the policy is fixed, and the science that supports it is promoted until the policy is Scientific(TM). I think most science-that-determines-policy is selected this way (regardless of the intentions of the scientists involved).
If I remember correctly you've mentioned this in a previous COVID post, where you recall that big scientific organisations are subject to all kinds of incentives and constraints, of which "tell the truth, the whole truth and nothing but the truth" is regrettably only one among many. I find this a much more productive lens through which to view policy debates compared to being endlessly frustrated that the Real Science with Actual Answers is not involved in the process.
comment by tkpwaeub (gabriel-holmes) · 2022-01-07T06:59:17.124Z · LW(p) · GW(p)
Speaking of risk factors - and I'll be mistaken for some weird variety of incel when I write this - why do we keep not taking sex into account when assessing risk for the purposes of prioritization of vaccines, medication, PPE, etc? We've known since the beginning that being male significantly increases the risk of mortality.
Replies from: CraigMichael↑ comment by CraigMichael · 2022-01-07T07:54:36.583Z · LW(p) · GW(p)
This is a good point. I don’t know if it’s changed with the variants, but believe that’s is unlikely as the mechanisms speculated were related to men having more ACE2 receptors.
comment by CraigMichael · 2022-01-06T22:50:30.647Z · LW(p) · GW(p)
Zeynep’s First Law
Can we start calling these Observations or Razors or something, but not Laws?
Usually people are like “ohh, well we mean ‘Law’ like Murphy’s Law not like thermodynamics.” But that cheapens something like this which is meant to be taken more seriously than “Murphy’s Law.”
During the height of the Gender Wars, “Briffault’s Law” was often rebutted by pointing out (1) the context it occurred in was an observation and (2) was not specifically about humans (although it was implied it could scale to them). This first bit of this rebuttal is only possible because the strength of the observation was either overstated as a “Law” (e.g. thermodynamics) in one context or understated in another (e.g. Murphy).
(I scanned Briffault’s book where he wrote the observation several years ago if you want to verify: https://archive.org/details/TheMothersTheMatriarchalTheoryOfSocialOriginsImages )
So much of the value in what could be a more valuable observation was lost because “we” obfuscated it by calling it a ‘Law’ when it wasn’t that in either sense. Let’s stop making this mistake.
So, I propose we call this: Zeynep’s First Razor
Replies from: gjm↑ comment by gjm · 2022-01-07T00:37:31.221Z · LW(p) · GW(p)
I also don't like "Law" for this, and cynically suspect that the use of "Law" for this sort of thing is at least sometimes at least partly an attempt to co-opt the prestige of actual laws while using "oh I just meant like Murphy" for plausible deniability.
It sounds as if you may be proposing "razor" as a general term for this sort of thing, which I don't like because there's a reason why Occam's Razor is called a razor rather than something else: it's a tool for trimming off low-value hypotheses. This particular proposition of Zeynep's is in fact razor-ish, though, so I endorse calling it a razor.
But "first" is ugly, and Zeynep doesn't use it. I suggest simply "Zeynep's Razor".
The "razor" formulation is better than "law" not only because it makes weaker claims to Universal Truth, but also because it correctly suggests a different kind of thing that this is: a methodological principle, of the form "consider these hypotheses before those ones". Of course the boundary between "consider these hypotheses first" and "... because they are more likely to be true" is a fuzzy one.
Replies from: Benito↑ comment by Ben Pace (Benito) · 2022-01-07T01:26:12.011Z · LW(p) · GW(p)
I note that I also like "Zeynep's Razor". Seems about as punchy as "Zeynep's Law" without slightly weakening the use of the term 'law'.
comment by PatrickDFarley · 2022-01-07T17:14:47.019Z · LW(p) · GW(p)
I also think that censoring that kind of statement is a reasonable thing to consider doing. But the rules seem to consistently get written in a way that does not differentiate between this and a similar true or good faith statement, and instead give power the ability to censor whatever they dislike.
This sounds to me a lot like "real X has never been tried," so my response is similar to what I'd usually say. This is what real censorship does. Censorship without falsehood is an unstable system bound to eventually reach equilibrium. Why? Because we live in a sufficiently social world that if you have censorship power, you can succeed without being right about the physical world (and why bother being right if it's slightly inconvenient?). Concentrations of social power attract simulacrum-4 players, and if they have enough power they can live whole happy lives without ever facing that rude awakening that the physical world exists.
“I am not seeing this movie because I don’t have to and you can’t make me.”
My thoughts exactly! And maybe it's because I've been reading these posts all along that I find the premise of that movie so exhausting; our institutions aren't set up to adequately handle crisis? No fucking shit. Apparently to many people this is a novel enough revelation that it makes for an interesting movie, which itself is frustrating.
My personal conversations have reflected what Scott said about the actual meaning being garbled. I haven't heard a real answer to this. So it sounds like some kind of "narcissistic ennui porn": Ennui because everything's fucked and we can't do anything about it; Narcissistic because, by being one of the rare few who recognize this, I'm special (never mind that I won't do anything about it); Porn because it's superstimulating and meaningless.
What's extra frustrating is to see it coming out of Hollywood, ie actual power. If you have 100+ million dollars, I don't want to hear about how "those in power won't listen to me about climate change!" Either you're not trying or you suck at being powerful.
comment by countingtoten · 2022-01-07T01:51:54.142Z · LW(p) · GW(p)
What do you think of this observation, which Leah McElrath recently promoted a second time? Here are some other tweets that she's made, on January 21 & 26, 2020:
https://twitter.com/leahmcelrath/status/1219693585731391489
https://twitter.com/leahmcelrath/status/1221316758281293825
Bonus link: https://twitter.com/gwensnyderPHL/status/1479166811220414464
comment by CraigMichael · 2022-01-11T17:29:50.775Z · LW(p) · GW(p)
Zvi - also usually you would post the data from the Bloomberg Vaccine Tracker. Which I think lives (or lived) around here somewhere? https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/
It doesn't load for me. Did you stop posting because of the same issue?
comment by Alexander Shmidt (alexander-shmidt) · 2022-01-11T02:02:30.894Z · LW(p) · GW(p)
Those are two options each with an expected value of $75, so I have no idea what decision making they plan to test there?
If you had exactly one shot, one opportunity to surely take $75 – would you capture it or would you let it slip?
comment by Oskar Mathiasen (oskar-mathiasen) · 2022-01-10T14:50:53.812Z · LW(p) · GW(p)
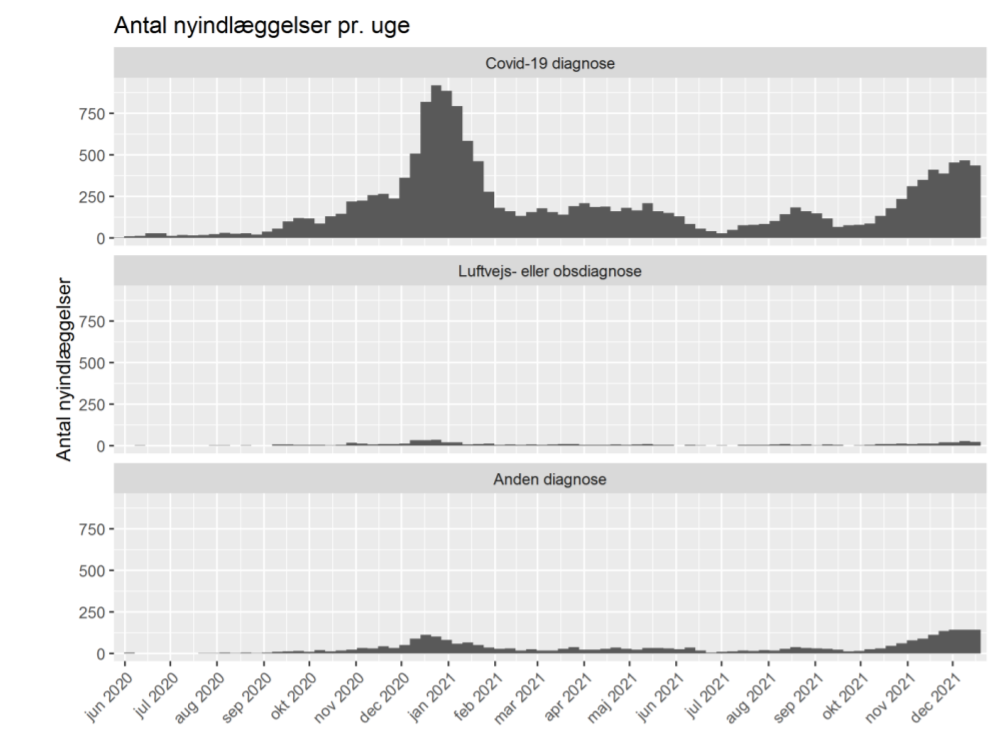
New report from Denmark called "Focusrapport about Covid-19 related hospitalizations during the Covid-19 pandemic"
https://www.ssi.dk/-/media/cdn/files/fokusrapport-om-covid-19-relaterede-hospitalsindlggelser-under-sars-cov-2-epidemien_06012022_1.pdf?la=da
It is sadly in danish, so i will give a translation of the main results section and some of the graphs.
Summary of main results:
Theme 1:
* The older a patient is, the greater the likelihood that he or she will have a covid-19- related hospitalization of 12 hours or more.
* The proportion of short hospital stays of less than 12 hours has been fairly stable in each age group in 2021 with a few fluctuations.
* The median duration of long hospital stays (≥12 hours) has decreased from 5.5 days in March 2020, to 4.4 days in February 2021 and 4.0 days in October 2021.
* (this one is added by me) The average duration of (long?) hospitalizations has decreased from 9.2 days in March 2020, to 7.8 days in February 2021 and 7.2 days in October 2021.
Theme 2:
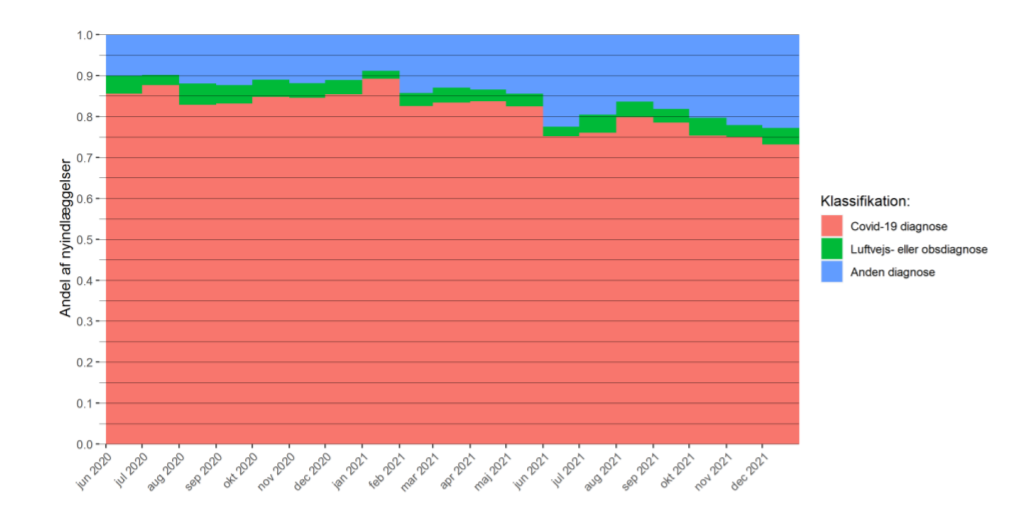
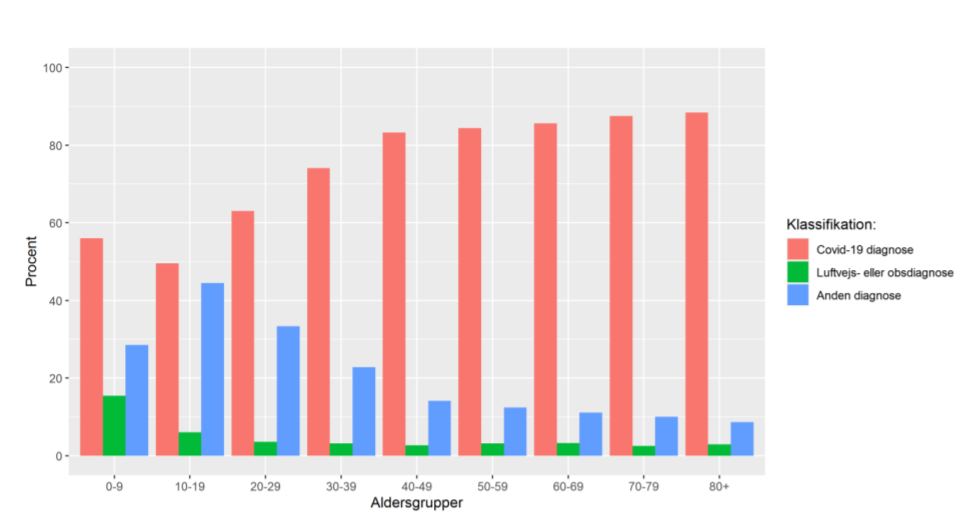
* Among covid-19-related admissions in the period 1 June 2020 - 18 December 2021, 82% were registered with a covid-19 diagnosis, 3% with a respiratory diagnosis or an observable covid-19 diagnosis and 15% with another diagnosis. In the month of December, December 1, 2021 to December 18, 2021, they were corresponding shares resp. 73%, 4% and 23%.
* For all age groups ≥40 years, at least 80% of the admissions were registered with a covid-19 diagnosis. For younger adults and children, the proportion was lower.
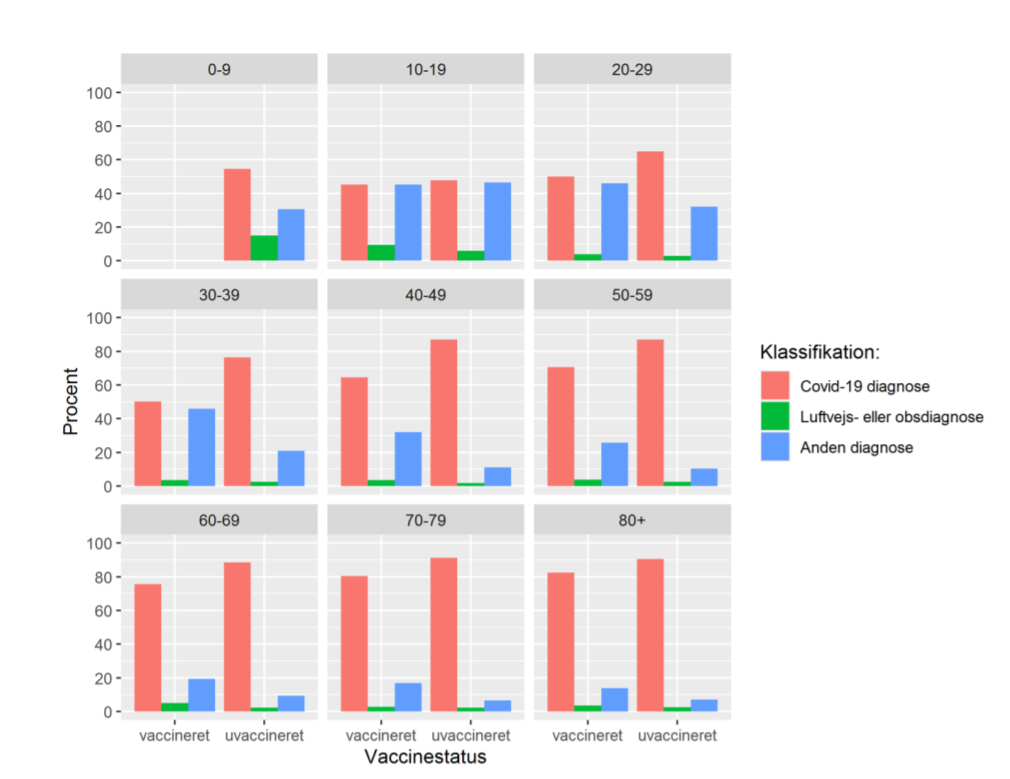
* For vaccinated, 75% of admissions were registered with a covid-19 diagnosis, while the proportion among the unvaccinated was 82% in 2021. The proportion of patients registered with a diagnosis incompatible with Covid among vaccinated and unvaccinated were respectively. 21% and 15%.
percent of covid hospitalizations which where longer then 12 hours (in red) vs shorter than 12 hours (in blue) by age group over time.

number of hospitalizations that are covid (top), airways or observation (middle), and other (bottom)
the above categories as a proportion of covid positive hospitalizations over time.
And the above categories as percentage by age group (over june-december 2021)
By age and vaccination status (vaccinated is to the left) (there are no vaccinated at ages below 9 in the period)
A few thoughts:
It seems weird that the median time of a long stay is going down, but the percentage of short stays is stable
comment by Craig Fratrik (craig-fratrik) · 2022-01-07T17:09:02.235Z · LW(p) · GW(p)
Small typo:
NYC Testing cites -> sites