Philosophy of Therapy
post by DaystarEld · 2020-10-10T20:12:38.204Z · LW · GW · 27 commentsThis is a link post for http://daystareld.com/philosophy-of-therapy/
Contents
I. History II. Case Study III. Modalities IV. Change the Frame, Change the Problem None 27 comments
For a lot of people, therapy can be a confusing, mysterious thing of questionable value. Many have tried it when they were younger, and felt that at best it was only of minimal help, while for others it actually made things worse. In many cultures, therapy looks very different from how it’s practiced in the “western world,” and the concept of mental health itself is often treated with suspicion or dismissal. I’ve known many people who, even while not being skeptical, were still confused about what the purpose of therapy actually is, or what situations warrant seeking a therapist out.
In my practice as a therapist, I often reorient myself to the basic core of therapy, which to me is about helping people get unstuck. Sometimes the thing you’re stuck on is a recurring and disruptive emotional state, other times it’s some harmful interpersonal dynamic, and other times it's a pattern of behavior. Whatever the specifics, there is some aspect of the client’s life that is not going the way they would prefer, and the therapist’s job is to help them find a way to change that.
What the therapy provides also varies; good therapy can create space for honest expressions of emotion, provide new perspectives or insight, and offer new “tools" for the client to use in their lives, specific behaviors or mental motions that help move past the stuckness.
Those skeptical of therapy often wonder: can’t people just talk to their friends or family if they need emotional support? Aren’t there self-help books they can try? And of course they can, and should try those things! For many people, the majority of their difficulties do not require a therapist.
Which means therapy is for what’s left. Those things that seem truly intractable, the things that you feel stuck on, which other resources have failed to help resolve.
But I’d like to demystify therapy further, and better yet, I think by better understanding what therapy is meant to do and how, people can get some of the value that therapy can provide even without going to see a therapist.
Because while much of the change in therapy comes from the therapeutic relationship itself (which is why first finding a therapist that you feel comfortable with is half the battle), for a large portion of clients I’ve seen, even just changing the frame of the problems they experience, or changing the way they view themselves in relation to their problems, actually makes the problem less sticky. A new frame can reveal more levers to pull and knobs to turn, or new vistas of the mind to explore and inhabit, that can help make the problem more manageable.
So that’s the goal of this essay. By teaching the history of the different philosophies of therapy, I want to teach you how, if you change the frame, you can change the problem.
I. History
Ask people to describe what therapy involves or “looks like,” and most who haven’t been in therapy will say something like “one person lies down on a couch and talks to the therapist, who takes notes and asks questions like ‘How does that make you feel’ and ‘Tell me about your childhood’ and ‘How do you feel about your mother?’"
This is largely the result of Hollywood Therapy, but it’s rooted in the origins of therapy, which is Freudian—what’s now called Psychoanalytic Therapy.
Sigmund Freud was the progenitor of applied psychology; the idea that we could study the way people think and feel and act, and use it to directly help them “improve” in some way. He was inspired by his mentor, a physician who helped alleviate a patient’s untreatable illness by just asking questions about her symptoms. That patient coined the term “talking cure,” and Freud took this concept and ran with it, dedicating his life to the idea that many ills people suffer are psychological in nature rather than physiological, and that just talking about them can help reduce or remove them.
Freud had a lot of ideas of his own, however, and while many them turned out to be nonsense, he also had some that turned out to be true, or at the very least, useful, such as the concept of a “subconscious,” or the idea of dividing a person’s mind into subagents (in his case, Id, Ego, and Superego). As the arrow above indicates, Freud cared almost exclusively about the past; he believed that by studying one’s childhood, the way they were raised, their early environment, or the origin of a certain dysfunctional behavior, you could identify all sorts of traumas or stresses that cause dysfunction later in life. Once identified, he believed the client would gain a feeling of “catharsis” that would start the path to healing.
Here’s where I admit that I have something of a bias against psychoanalysis.
In my view, Freud was a philosopher first and foremost, rather than a scientist. He had interesting ideas that seemed logical to him, and a scientific frame of mind, but while he pursued the application of these ideas with an admirable gusto, his documentation did not seem to aim its rigor at testing which of his ideas were true. I'm unaware of any hypotheses Freud generated that he then went on to falsify. (If you know of any, please do share them!)
Far from an attempt to bash the man, I do admire him a great deal. It’s hard to be the first person to basically invent an entire field of science and do it all perfectly such that you are simultaneously the person observing reality, coming up with ideas, and dispassionately testing those ideas, all while trying to do work as a clinician. But I believe most modern schools of therapy have picked out the gems of his work and left the rest to history lessons.
That isn't to say this branch of therapy is all worthless. While catharsis alone generally doesn't solve most people's symptoms (psychosomatic illnesses like his mentor's patient's are in fact very rare), delving into one’s past can lead to insights into their current problems, and many do report feeling better about their problems when they have a chance to talk about them (again, credit to Freud, this would likely have been very encouraging to him when he began his work).
Additionally, as a colleague pointed out to me after reading an earlier version of this article, many modern psychoanalysts do seek to empirically test the field's ideas in order to continue to develop evidence-based treatments, and modalities such as Transference-Focused Psychotherapy have evidence suggesting it to be at least as effective as other standards of treatment.
(A modality is a method of therapy that has a specific structure to help a client reach wellness. More than a specific intervention, modalities often include multiple interventions, as well as a particular type of relationship between client and therapist that dictates whether the therapist acts as more of a guide, partner, or authority. Each modality operates on a particular hypothesis of how therapy can help clients with certain problems.)
In any case, while psychoanalysis as practiced by Freud and his ideological descendants (Carl Jung, Anna Freud, Erik Erikson) focused so much on the client’s past, new discoveries in psychology led to therapeutic modalities that focused instead on influencing the client’s future.
Enter, the Behaviorists.
As Freud is to Psychoanalysis, so Ivan Pavlov, of dog fame, is to Behaviorism. Pavlov discovered and experimented with classical conditioning, the idea that you can pair different stimuli to influence responses. This discovery was a great boon to pet owners, but also has direct applications to therapy. One example is addiction treatment, where for example the sight or smell of cigarettes or beer is paired with something that will evoke disgust. It also led to desensitization therapy for phobias, where pairing progressively more frightening stimuli with techniques and context that help relax the client can alleviate the fear response.
These ideas were expanded by Edward Thorndike and B.F. Skinner, whose work is called operant (or instrumental) conditioning. Rather than just pairing stimuli together to affect responses, their experiments showed demonstrable effects on learning and behavior through reinforcement and punishment; in therapy the idea of using positive reinforcement to incentivize desired behavior is often helpful for children, particularly those with developmental issues.
I don't have much to say about Behaviorism. For some things that people come to therapy for help with, it just works. For others... not so much. I think understanding the mechanisms of Behavioral Therapy is valuable for any clinician, but there's some obvious flaws with taking it as the only avenue toward better mental health.
Unlike psychoanalysts, a straw-Behaviorist doesn’t care about your past, and talking about your traumas or “deeper issues” would often be considered a waste of time. Instead the focus is on your symptoms. No symptom, no problem, right? Just apply the right type of reinforcement to increase positive behaviors and the right type of punishment to decrease negative behaviors, and all’s well…
…for some people, at least. Behaviorists had a lot of success in some domains, particularly when the “why” of the problem didn’t actually matter to the client or issue, but obviously struggled with others. After the first World War, clinicians formally recognized PTSD, or "shell shock," for the first time. Unfortunately, attempts to treat soldiers through psychoanalytic and behavioral therapy often failed, and so many psychologists turned clinician to help figure out how better understanding the present feelings we have, and how they impact our behavior, can lead to mental health.
Which brings us to Existential Therapy.
Rather than having a single founder, the Existential philosophy of therapy was converged upon by a wide range of psychologists and clinicians, many inspired by the writings of Kierkegaard, Nietzsche, Husserl, Scheler, Heidegger, and Sartre. These writers’ attempts to redefine our understanding of not just what it means to be human, but an “actualized” human, a healthy, thriving, happy human, were believed to have great value in clinical efforts to help those in need.
But among that foundational pantheon, the first of the Existential therapists was Otto Rank, a student of Freud who later split with him over Freud’s beliefs that a person’s “formative years” are what determine who they become. Instead, Rank believed that human development continues throughout our lives, requiring continual negotiation and renegotiation between dual yearnings for individuation and connection.
For such heresy he was excommunicated by the psychoanalytic world, but he nevertheless influenced his own “family” of psychologists, including Rollo May, Viktor Frankl, who's more well known as the author of Man's Search for Meaning, and Abraham Maslow, of hierarchy fame. These psychologists focused not so much on what happened in someone’s past or how to influence their future, but on their now. What do people feel like they need, that they lack? How does the client experience “need” at all? What relationship do they have with their hurts and wants, and what would be necessary for them to feel fulfilled? How do those different needs and wants conflict with each other, and how can they be better brought into harmony?
Existential therapy also marked a new dynamic between client and therapist; rather than a top-down hierarchy, where the clinician is the “expert” and the client the “patient,” what became known as client-centered therapeutic practice began to form. It placed both therapist and client as equals; the clinician has the education and skills, but the client is the expert on their own lives, of what they think and feel, and so the Existential therapist’s role is more that of a facilitator to the client’s growth.
This may seem like polite semantics, but most people who’ve been to both kinds of therapists can tell how big a difference it makes if, upon disagreeing with their therapist on something, they’re treated not like a stubborn mule who is “resistant” to change, but rather a person with agency, whose motivation to improve is taken for granted by their therapist. The philosophy also emphasizes the importance of a therapist who is willing to listen, encourage, and support the client’s personal journey to better mental and emotional health, as the client defines those things.
Under the light of Existential Therapy (and its more upbeat twin, Humanistic Therapy) there grew many techniques to help clients better understand themselves, including Carl Rogers’s “reflective listening,” which has become a staple of good therapy from every philosophy, as well as techniques to better interface with our emotions, such as “focusing” by Eugene Gendlin, which I personally have found to be one of the most generically effective tools to teach practically every client I've had.
Time to admit to another bias, in case it's not clear; I’m a huge fan of existential/humanistic therapy. In my experience it has a wide “range” in what it can successfully treat, and its frame makes up an integral part of what makes modalities effective in general.
But it’s not the form of therapy I was formally educated in, and it’s not the latest form of therapy that was developed. There’s one last dimension that even existential therapists failed to engage in, and if you’re following the theme of the arrows you might have guessed it: the opposite of focusing on ourselves is focusing on everything else.
Enter Systemic Therapy (also known as Family Systems Therapy, or just Family Therapy), born in the 1950s from a very powerful need; the need for better marriage counseling.
In the post WWII era, if a husband and wife wanted to save their marriage, they would go about it thusly: the man would have his counselor, and the woman would have her counselor, and both would see their counselors separately. If they went to a fancy clinic dedicated to marriage counseling, the two clinicians would be coworkers, seeing their clients individually, then consulting on the case between sessions, or even mid-session before returning to their clients.
If that sounds crazy, just remember that this was the 50’s, when people still thought smoking was good for you. The idea was that a client’s relationship with their therapist was sacrosanct, and must always be preserved as a space of utter one-on-one privacy that would allow them to be completely frank, without worrying about their spouse’s presence, or their therapist telling their spouse anything spoken of in confidence.
Eventually some therapists in California realized how absurd this was, not to mention ineffective. They suggested a new way to practice marriage counseling, where a single counselor (or even two) spoke with both clients together, in the same room and at the same time. That way a therapist could observe their interactions and mediate their discussions directly.
Their clinic said no.
So Don Jackson and his colleagues left to form the Mental Research Institute in Palo Alto, where they developed their own modality of therapy, one that involved not just the individual patient, but sometimes romantic partners, family members, even friends if the problem called for it.
They weren’t the only ones; Salvador Minuchin, Murray Bowen, Ivan Boszormenyi-Nagy, Virginia Satir, and Jay Haley all developed modalities based on the idea that, to help a client overcome dysfunction, the therapist should focus not just on the client, but the system they’re a part of, whether that be their family, their work environment, their culture, or even their country, all at various levels of abstraction.
(There isn’t going to be a test on all the names I’m throwing at you, but if I went into every single modality we’d be here all day, and this way you have an easy way to look into them on your own if you want.)
The study of cybernetics and communication theory were also prominent influences, particularly by the anthropologist Gregory Bateson, who believed that all forms of communication are adaptive, and rejected the concepts of linear and dualistic thinking for studying systems.
The “systems” being referred to in these therapies can be any context you’re a part of, individually or simultaneously: family system, school system, work, friend-group, even cultural and religious. According to Bateson, being part of any system leads to inherent and unavoidable communication between you and the other parts, implicit or explicit, which affects the other parts of the system and how they behave, which further affects how you behave, and so on. Additionally, there can be no divide between an interactive observer and participant of a system; by observing the system directly, the therapist becomes a part of it.
This understanding led to a philosophy that takes the humility of existential therapy even further, and improved clinicians' ability to map the impact of one part of a system on the others, such that many modalities do not even identify anyone in particular as “sick” or “healthy,” but rather views behavior patterns themselves as dynamic or stagnant, and focuses on how change can propagate through the system by nudging elements of it. By understanding how everyone’s actions and reactions affect each other’s behavior, the client and clinician have more surface area on the problem to try and find solutions, more levers to pull and handles to grip from.
A big reason why this lens can be so valuable is that when you start working with groups rather than individuals, you have to address the fact that often times, not everyone involved in therapy has the same desire to be there, let alone incentive or drive to change. Of course, that was true before couples or entire families were being invited into a therapy room at once, but now the therapists were actively working to address it rather than just assuring whoever cared enough to be in the room that the problem was other people, and not them.
Oh, also worth noting that therapy up to this point was still a LONG process, often expected to last years. Systemic Therapy made a push toward briefer, more effective interventions, creating modalities like Solution Focused Therapy, which combined Systemic and Behavioral principles to bring about real, lasting change within 4-6 months.
So, that’s the four cardinal philosophies I’ve sort-of-made-up as a labeling scheme to map all therapy onto. Now we get to the meat of the matter; how can just knowing about them actually help?
II. Case Study
“You have to help me,” Marge, 55, says during her first session. “It’s my husband. He’s become obsessed with model trains!”
Sidebar 1: An important thing to note is that the client said she needs help, but highlighted her husband as the focus of therapy. Some equivalent of “fix my spouse” (or “fix my kid”) is nearly as common, in my experience as “fix me,” and often times the spouses in question aren’t always in the room. So we work with what we have.
“I can see you're worried about him," I say. "What does ‘obsessed’ look like? Are you running out of money?”
“Well, no,” she admits. “We can afford it, but… every month he’ll order hundreds of dollars worth of new models and tracks, and after work he goes down to the basement. He spends hours down there, every day!”
I nod. “Yeah, it makes sense why that might be concerning. Is he skipping meals? Staying up all night?”
“No, no. He’s sleeping fine, he’s still eating… but it’s quick, you know, he’ll pop out of the basement for ten minutes, wolf down his food without looking at it, then go back to his trains for another six hours. That’s not normal, right?”
Sidebar 2: “ Normal,” along with “healthy,” is perhaps the most loaded word in therapy. Unless the client is insistent, or we’ve formed a strong therapeutic relationship, I try to avoid giving any kind of verdict on either, and instead use the therapist standby of answering a question with a question; in this case not ‘what is normal,’ but rather:
“What would you consider to be the ‘normal’ things he does do?”
“You mean like work?”
“Yeah, and beyond that. Is he still seeing his friends?”
“Yes, once in a while he’ll go out for some drinks with them.”
This is evidence that he’s not a shut-in. “Feel free to say it’s too personal for now, but just to check, does he still want sex?”
She blushes. “Not often, but, yes. Sometimes.”
“Okay. Does he talk about other things, or is it all trains all the time, now?”
“We barely talk at all, now, not like we used to.”
“What was the last conversation you had with him?”
“Oh, about the kids.”
“You have children?”
She smiles for the first time. “Yes, two. Both married, one with our first grandchild on the way.”
“Congratulations! And he’s still interested in them, and the grandchild?”
“Oh, yes. He put off our vacation so we’d be around the first few months.” Her smile is gone now. “Which normally I’d be in favor of too, but… there’s some sort of convention nearby around then that he’s still planning to go to.”
“A model train convention?” I guess.
“Yes, I’m telling you, he’s just…” She shakes her head, seemingly at a loss for words.
Sidebar 3: “Pathologizing” is the perception that any action or view that is unusual is automatically a sign of illness, despite no evident dysfunction or suffering. In decades past, previous versions of the Diagnostic and Statistics Manual labeled things like homosexuality a mental health illness due to a mentality that didn’t distinguish between “normal” and “healthy.” Newer versions of the DSM have eliminated most of those, and there’s a concerted effort among (good) psychologists and therapists to distinguish real pathology as something that causes direct suffering for the patient.
At this point, I might feel an urge to say “Okay, so… what exactly is the problem here? Just because your husband is spending hundreds of dollars and hours a month on model trains doesn’t mean he needs therapy. If it’s not affecting his sleep, or his appetite, or his work, or his social life… maybe he just likes trains, and that’s okay? It’s far from the worst hobby, and if it makes him happy, just let him like trains!”
I wouldn’t say this out loud, however, at least not in the first session, because even if I’ve become at least reasonably sure that the husband is okay, to say something like that would be dismissive of her experiences .
Regardless of what her husband is doing, she is clearly unhappy. And while she might think she can be the client but not the patient, the truth is, from a systemic lens, there is no distinction. The system she lives in, her marriage, is clearly dysfunctional for her in some way, as evidenced by how she’s suffering enough to come to a therapist. Perhaps her husband is too, in a non-obvious way that will be revealed through further questioning, but for now the focus would best be shifted to her.
There are a number of lenses through which to focus, however, and each might approach the problem in such different ways that they essentially become different problems .
- A psychoanalytic therapist could delve into Marge’s past. Was her father distant with her, perhaps obsessed with his work or a hobby of his own? Did she have older siblings that left her out of their play? Was a childhood friend killed by a train? (Probably not that last one.)
- A behaviorist could focus on the husband’s actions and develop strategies to reinforce or punish the ones she likes/dislikes. This would be pretty manipulative if the husband isn’t on-board, however, so instead the therapist might focus on ways to associate her husband’s hobby with positive emotions and experiences of her own.
- An existentialist could help Marge delve into the emotional experiences she’s having, what she feels when she thinks of her husband in the basement or buying new models, and what needs she has that aren’t being met. The goal would be either to dissolve the problem entirely by reframing her expectations, or teaching her new tools to manage her mood and satisfy her emotional needs.
- A systemic therapist could help by examining the overlapping systems she’s a part of; her marriage, her family, her social circles. Did she and her husband used to do more things together? What was their marriage like when the kids were still part of the household? How often does she spend time with her own friends or hobbies? Perhaps there are ways she could better communicate to her husband what her needs are so he can understand how she's hurting, or examine what behaviors of hers might be reinforcing her husband’s without even realizing it.
While individual modalities might lack scientific backing, I believe the broader philosophies can each be suited to different types of problems. That still means that if a therapist only sees the world through one or two lenses, they might not be able to help their client as well as someone whose approach is the better fit.
Perhaps more importantly, each client can respond better to a different philosophy, even if they present with nearly identical problems. For some, just getting down to brass tacks and tackling the symptoms is their ideal, while for others, digging deep into their psyche is what they want and respond well to.
This is part of the reason why one of the major tenets of good therapy is “stay curious.” The more the therapist starts assuming they know what to expect from a client based on their presenting problem, no matter how often they’ve seen it before, the more likely they are to jump to conclusions about treatment that end up being a poor fit.
III. Modalities
A therapy modality is more specific than a philosophy; it’s not just a framework for what leads to dysfunction and how to correct it, but also a bundle of specific interventions and pathways, some more rigid than others, to lead the therapist and client from first session to last. Here’s just a few examples that I use regularly:
Cognitive Behavior Therapy is a mix of Existential and Behavioral. It focuses on the looping interactions between our thoughts, feelings, and behavior, and how they reinforce each other such that altering one can alter others. (Dialectic Behavioral Therapy leans even more into the Existential side, with extra attention on mindfulness and mood regulation.)
Solution-Focused Therapy is a mix of Systemic and Behavioral. It helps the client identify their strengths and resources in their social systems, as well as how those systems reinforce their behaviors or symptoms, or can be altered to better reinforce more desired ones.
Narrative Therapy is a mix of Systemic and Existential therapy. It asks the client to present the narrative of their life, identify the ways the story they tell themselves and its framing is influenced by the broader systems they’re a part of, then explores the way their narrative makes them feel while teaching techniques to better interface with those feelings.
And here’s a handy-dandy diagram that lists just a few of the different modalities, techniques, and interventions used in therapy. There are many more that exist, and there may be different ways of practicing each of these that bump them from one section of the diagram to an adjacent one, but I believe every modality and strategy of therapy can ultimately be placed somewhere on this image, depending on how much they focus on understanding the client’s past, interfacing with their thoughts and emotions, altering their behaviors, or adjustments to their environment/relationships.
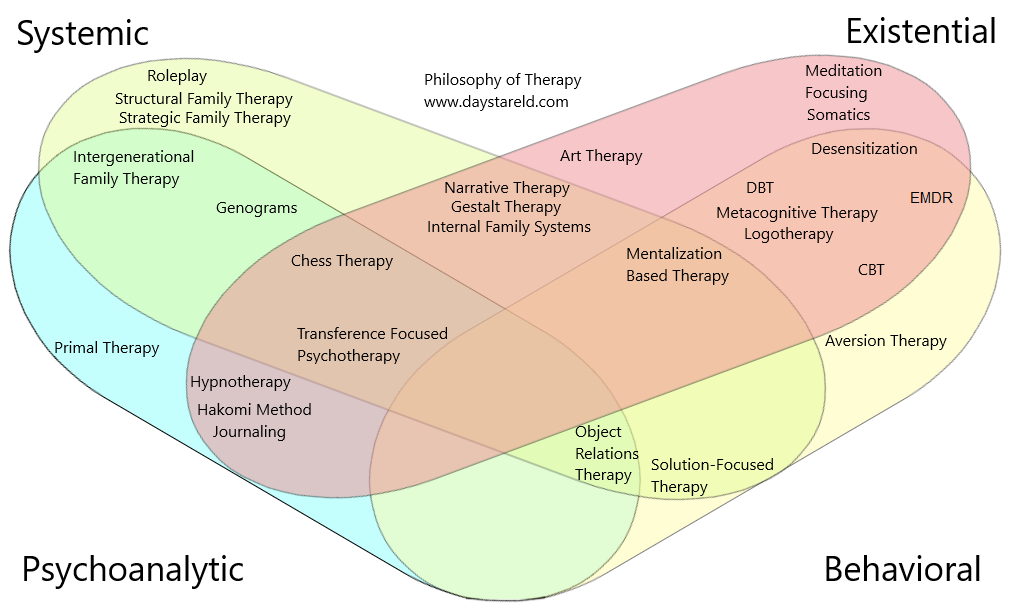
(This is in no way a "complete" image, as there are dozens of different modalities and it would need to be massive to fit them all, but I figured it's better to just publish with some listed and update it over time.)
IV. Change the Frame, Change the Problem
I like collecting lenses through which to view the world. Each is like a different kind of mental map that I can use to navigate the territory of reality, and just like different types of maps (some simplistic and cartoonish, others realistic and highly detailed) can be more or less useful for different purposes, even maps that I know are not literally correct can still have value.
Overall this post is an ur-map, my ur-map, of different maps I’ve learned about in the field of therapy. I don’t mean to present it as “the one true way to view therapy,” but I’ve found it very helpful, and I hope others can too. It’s also worth keeping in mind that it has many of the biases you’d expect from someone educated in an American college program that focused primarily on one particular philosophy.
Still, I think if more people were aware of the different lenses through which therapy can operate, they would better be able to navigate the sorts of problems that might lead them to a therapy office, maybe even help them find their way without going to one.
Next time you feel stuck in a particular way of thinking about your problems, a particular frame through which your problem seems insurmountable, try changing it. You might find it a lot more tractable than it seemed before.
27 comments
Comments sorted by top scores.
comment by remizidae · 2020-10-11T18:54:53.504Z · LW(p) · GW(p)
What I was expecting from the first paragraph was a discussion of whether therapy works. I think people should know that when it's been studied, there's little evidence that talk therapy works better than getting support from a friend, family member, or other trusted person. A person with a credential, some insight, and an empathetic manner is not clearly better to talk to than a person with some insight, an empathetic manner, and no credential. And it's important to remember that therapy comes with significant costs in money and risk. Anyone who gets involved with the psychiatric system should be aware of the substantial risk of overmedication and medication side effects, as well as smaller but still real risks of involuntary medication and institutionalization.
To address some common objections:
1) But therapy worked for me!
Response: Maybe. But anytime a person invests substantial time and money into a given strategy, there is a risk that their assessment of the results of that strategy will be affected by confirmation bias, sunk cost bias, and cognitive dissonance.
Also the post hoc ergo propter hoc fallacy: I was depressed, then I went to therapy for six months, now I'm not depressed. Great, but most cases of depression resolve after six months, with or without treatment. How do you know what would have happened if you had tried some other strategy, or nothing at all, for six months?
2) But I don't want to/can't get a friend to listen to my problems for an hour+ a week, and a therapist will.
Response: Are you sure you need to talk about your problems for that long that often? Or is that just what the psychiatric establishment has taught us is standard?
Experiment for yourself, by all means, but my experience has been that a very brief conversation, coming at the right moment, can be incredibly therapeutic. Or an in-depth conversation every few months. Or support from a friend along with all the other self-help strategies that commonly work for mental/emotional problems.
3) If you tried therapy, you would see how great it is. Therefore, you must not have tried it, so I will dismiss your opinion.
Response: This is a dumb ad hominem, but it seems to come up every time I make this point, so I will address it. I've done a LOT of therapy, with a lot of different people, for a range of different problems, and it never worked. Put very little weight on this, of course, it's very possible that it didn't work for me but will work for you. I only bring up myself to foreclose the ad hominem.
Conclusion: if you're considering therapy, be aware of the costs and benefits. And know that it's not your only option, and it is one of the more costly options out there.
↑ comment by DaystarEld · 2020-10-11T20:18:44.267Z · LW(p) · GW(p)
Let me start by saying that I definitely don't recommend people go to therapy anymore unless I can also offer them guidance (like with this post) in what to expect or how to spot a good therapist or what kinds of modalities are effective. There are just too many bad therapists out there. But I think your comment may be too confident in the wrong direction.
>I think people should know that when it's been studied, there's little evidence that talk therapy works better than getting support from a friend, family member, or other trusted person.
Would love to read a source for this, if you could point me to which study you're referring to. To me the most interesting studies on therapeutic effectiveness focus on a particular modality, like the one I linked to in the post, whereas "therapy" as a whole is such a mixed grab-bag of different philosophies and ideas that as a generic practice, I'm definitely willing to believe that most people's experience with it has not been particularly effective. But that doesn't mean an "informed shopper" with a good guide can't beat the odds.
>But anytime a person invests substantial time and money into a given strategy, there is a risk that their assessment of the results of that strategy will be affected by confirmation bias, sunk cost bias, and cognitive dissonance.
Interestingly, my experience is the opposite; people are very quick to point out when therapy didn't work for them, particularly if they feel like they wasted a lot of time and money at it. I don't generally see a lot of people singing the praise of therapy unless they had an outstandingly good experience with it.
>Experiment for yourself, by all means, but my experience has been that a very brief conversation, coming at the right moment, can be incredibly therapeutic. Or an in-depth conversation every few months. Or support from a friend along with all the other self-help strategies that commonly work for mental/emotional problems.
Absolutely true, for the majority of situations people are troubled by. As I said in the post, I think therapy is best meant for when nothing else seems to work, including talking to friends and family.
>If you tried therapy, you would see how great it is. Therefore, you must not have tried it, so I will dismiss your opinion.
This is indeed a dumb argument, and I'm sorry that you've been told that. Like I said, I've often heard the opposite; people with bad experiences with therapy are more likely to speak out about their bad experiences, in general, and most get sympathy for expressing how therapy didn't work for them. I can imagine people trying to suggest that THEIR experience with therapy was particularly good and so if you just tried the modality they experienced maybe you'd change your mind, but practitioner skill also makes a huge difference, and the relationship with the practitioner is always a wildcard, so people should generally be a lot less confident when recommending therapy to others.
That's a large part of why I made this post; to help people get some benefit from therapeutic philosophies without having to necessarily go to a therapist themelves.
↑ comment by maia · 2020-10-22T13:13:02.660Z · LW(p) · GW(p)
One part of your post jumped out at me as something that's hard to reproduce without therapy:
> Experiment for yourself, by all means, but my experience has been that a very brief conversation, coming at the right moment, can be incredibly therapeutic. Or an in-depth conversation every few months. Or support from a friend along with all the other self-help strategies that commonly work for mental/emotional problems.
Getting help from a friend at the right moment can be very helpful. But sometimes your friends aren't available at the exact right moment, just because of things in their own life or whatever. The nice thing about paying a professional is that you're paying for reliability. If you can't find someone to talk to when you really need it on a given week, at least your therapist will be around.
↑ comment by romeostevensit · 2020-10-12T05:46:36.146Z · LW(p) · GW(p)
I agree with this and think people setting up peer counseling with a friend is high leverage. This means that one meeting/week is mainly focused on you and your problems, and one day a week the meeting is focused on them and their problems.
↑ comment by gwern · 2020-10-13T00:22:47.766Z · LW(p) · GW(p)
What I was expecting from the first paragraph was a discussion of whether therapy works. I think people should know that when it's been studied, there's little evidence that talk therapy works better than getting support from a friend, family member, or other trusted person.
Better known as the 'dodo bird verdict'...
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2020-10-13T02:00:28.574Z · LW(p) · GW(p)
Wikipedia defines the dodo bird verdict as "the claim that all empirically validated psychotherapies, regardless of their specific components, produce equivalent outcomes", which is noticeably different than "talking to a friend produces equivalent outcomes to therapy". They can both be true, but I don't think they're the same thing.
Similar definitions from study.com, Scientific American, some journal
Replies from: riyad-parvez↑ comment by Riyad Parvez (riyad-parvez) · 2021-01-08T17:26:12.862Z · LW(p) · GW(p)
the claim that all empirically validated psychotherapies, regardless of their specific components, produce equivalent outcomes
I think when you aggregate the difference in effectiveness between different schools of therapies for different sorts of mental illnesses fades away. The reality is different schools of therapy are good for different types of illnesses, disorders or just unhappiness in general. I can see CBT being helpful in some cases. But I find the notion that someone, who has been abused for years during their developmental period, can be cured or even improved by few months of very structured and (simplistic) CBT therapy sessions is simply preposterous. For very simple truma I can definitely see CBT or similar manualized therapy being effective. For complex trauma, you will need years of comibnation of relational, interpersonal, humanisitc, existential, psychodynamic, somatic or neuro-science based therapy.
To sum up, it all depends on what kind of issues clients want to resolve. Specific types of therapies will be more effective for specific types of issues.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2021-01-09T00:02:57.134Z · LW(p) · GW(p)
I'm confused why this is a response to my comment, which was not an argument for or against the dodo bird verdict but about definitions.
comment by Kaj_Sotala · 2020-10-18T09:39:16.856Z · LW(p) · GW(p)
Curated.
I have generally been of the view that therapy is important for rationality [1 [LW · GW], 2 [LW · GW]], and this articulation of the goal of therapy as being about "getting people unstuck" feels like a framing that is particularly compatible with the rationalist project: after all, if "rationality is about winning", then getting unstuck and solving your previously-unsolvable problems is quite necessary for winning!
I generally liked getting a historical look at how therapy has evolved and what might then be called the "approaches for getting unstuck", and particularly appreciated getting it from someone who's actually a trained and working therapist - a profession I'd like to see represented more on LW. Though the post could have gone into more detail on it, the four philosophies suggest four different ways for trying to solve your own problems [LW(p) · GW(p)], which I expect to be helpful for e.g. people looking for a good therapist or ideas on how to solve their issues.
comment by ozziegooen · 2020-10-11T02:04:10.082Z · LW(p) · GW(p)
Thanks for this, I found it an interesting overview.
I would note that I found the title a bit confusing. I would have suggested a more descriptive name, maybe something like "Modalities of Psychological Disciplines" or something more to the point.
Replies from: DaystarEld↑ comment by DaystarEld · 2020-10-11T20:06:50.885Z · LW(p) · GW(p)
Glad to hear it!
Yeah, I know the title is a bit vague, but Modalities are pretty specific and only like 1/3 of the post if that focuses on them. I've thought of alternative titles, like "Change the Frame, Change the Problem," but that's pretty vague too, and nothing feels like it fits better.
↑ comment by ozziegooen · 2020-10-11T22:10:34.586Z · LW(p) · GW(p)
It's probably too late to change the title of this, but I'd press back against that a bit.
To me, the "Philosophy of X" typically refers to an entire academic field of study. Philosophy of Physics, Philosophy of Science, Philosophy of Psychology, which is a distinct thing.
My guess is that this wasn't your intention, but calling this "Philosophy of Therapy" could be read as you asserting that this post represents an overview or beginning of a similar field.
I could imagine the naming being fine on your blog, but LessWrong is quite big. If I were to point someone to the "Philosophy of Therapy", I'd expect something different, and think they would too.
Replies from: DaystarEld↑ comment by DaystarEld · 2020-10-12T08:57:59.634Z · LW(p) · GW(p)
Since there's currently no academic field of study on therapy as a whole, I would argue that the contents of the post would be a reasonable starting point in forming one, or at least that it covers a lot of the same material (what therapy strives to do, what the base assumptions are, the various different theories of change that different therapy schools hold, setting out a system of classifying modalities, etc). I don't think the post meets the rigor for a published paper, and such an academic field ideally would be focusing on studying effectiveness of each philosophy/modality, but it's not unrelated to what I imagine a hypothetical Philosophy of Therapy field to focus its attention on.
If you disagree, could you say a bit more about what you would expect such a post using the name in that context to contain?
comment by frontier64 · 2020-10-28T00:21:25.541Z · LW(p) · GW(p)
Thanks for your enlightening post, I feel like it helped me kind of build a broad outline of therapy. I have a question about how much info a non-therapist should have about therapy: Do you think there's educational value in reading patient case studies as a lay person? And a more specific version of that general question: could reading case studies on a particular pathology help me better understand and empathize with my friends, acquaintances, and other people I meet who have a trait which is a less severe form of that pathology?
From my subjective experience:
I have a high school friend, Bob, who is well known--among both our mutual friends and his friends whom I've only met rarely--as a habitual liar and over-exaggerator. Throughout high school and for many years of knowing him afterwards I would more and more often respond to his lies with scorn, and occasionally gossip with others about him, and in general had a lesser opinion of him than I would have had otherwise. Within the past year I read a few case studies on pathological lying and it's actually helped me empathize with him quite well.[1] I had heard about and had a rough definition of pathological lying before, but I wasn't quite able to internalize that knowledge until I read the case studies.
I saw many of the same behaviors described in the pathology in Bob. But the most important takeaways for me from those case studies are the proper ways to peacefully coexist with Bob and a greater ability to empathize with him now that I have non-malicious theories to explain his behavior. Overall it's improved my opinion of him significantly and allowed me to speak with him again with significantly less tension.
A similar thing has happened with one other friend and reading case studies on a different pathology.
I want to be clear that I am not predicting that any of my friends have disorders; Bob's propensity to lie hasn't negatively affected his life too badly from what I've seen beyond him losing a few friends because they were very sensitive to lying. But I've heard that you can view pathologies as the extremes of personality traits.[2] If so then it would stand to reason that studying a personality trait at one extreme can give you a glimmer of a similar personality trait in moderation.
I still see a non-negligible chance that my behavior here could be a mistake and that reading a case study and viewing a friend as a less extreme version of the patient in that study is just as bad as pathologizing.
I've seen it referred to as "pseudologia fantasia" as well. Apparently it's not a listed disorder, but still treated as one by some psychologists? https://pubmed.ncbi.nlm.nih.gov/12108140/. ↩︎
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4125199/ I'm not sure if this is widely accepted or up to date. ↩︎
↑ comment by DaystarEld · 2020-10-30T00:34:51.638Z · LW(p) · GW(p)
Good questions. I think that there's definitely value that comes from reading case studies, especially for learning to live with someone who has the same diagnosis. I'm particularly thinking of things like addiction or trauma or anxiety/depression, but it applies to personality disorders as well.
But yes, the risk of pathologizing is there if the person hasn't actually been diagnosed. To counteract this, noticing what's working in the client's life can help, as noted in the hypothetical case study above.
comment by PatrickDFarley · 2020-10-12T22:43:06.527Z · LW(p) · GW(p)
I found this extremely helpful. I'd known the world of therapy was complex but I had nothing like a broad map of it.
After staring at your chart for a minute I noticed that there are some modalities I'm able to do well for myself, and others that I'm not. When people claim they wouldn't benefit from "therapy," they're likely thinking of one or two modalities (and are likely correct), but may not be aware of the others.
Replies from: DaystarEld↑ comment by DaystarEld · 2020-10-13T08:25:37.492Z · LW(p) · GW(p)
Yes, I think a big part of what ends up happening when people have bad experiences with therapy is that they imagine that the therapist they had, or the type of therapy that therapist practiced, is representative of all therapy. This may actually be true in some parts of the world, but in countries like the US there is a huge variety in both modalities and therapeutic "personalities" so to speak.
comment by Kaj_Sotala · 2020-10-13T15:44:31.216Z · LW(p) · GW(p)
What would you say would be one-sentence (or one paragraph) descriptions of the "main principle" behind each philosophy that you've covered?
Extracting what I got from your descriptions, it might be something like:
- Psychoanalytic: Discuss your issues in relation to your past.
- Behaviorist: Apply reinforcement to increase positive behaviors and punishment to decrease negative behaviors.
- Existential: Come to better understand your current experience and needs.
- Systemic: Understand and change how you are affected by the patterns of the system that you are in.
↑ comment by DaystarEld · 2020-10-16T06:24:39.746Z · LW(p) · GW(p)
Pretty good :) My versions just kept tweaking what you already wrote, except for Systemic, to which I would also add "and how you affect that system." A lot of systemic therapies explore not just how the system might be perpetuating the pathology, but how the client's behavior also maintains that system, such that it perpetuates the pathology, recursively.
comment by philip_b (crabman) · 2020-10-13T11:25:59.449Z · LW(p) · GW(p)
When I saw the title "Philosophy of therapy", I hoped to find some answers to the following questions:
- How to think about therapy given Dodo bird verdict?
- How to think about therapy given that approximately 50% of all published studies in it fail to replicate?
- Given 1 and 2 and the fact that therapy works for some reason and the fact that different types of therapeautic theories contradict each other, therapy must work not only because because it improves the patient's map of the territory, but also by another mechanism. So, what's going on here? Maybe it improves the patient's map of the territory despite the incorrect information in therapeautic theories?
↑ comment by DaystarEld · 2020-10-16T05:41:45.215Z · LW(p) · GW(p)
For one thing, the Dodo bird verdict is (maybe not surprisingly, given point 3) not as well supported as people widely think. It originated decades ago, and may have set in motion the very effects that led to its own eventual lack of relevance. The study I linked to in the OP, if correct, points to just such an invalidation by presenting findings that a particular modality works better for a certain type of treatment than alternatives.
But if we take it at face value, the answer could just come down to "the human element." Maybe good therapists are what matter and the modality, as long as it's not utterly bankrupt, is just a vehicle. Personally I don't believe that's the full story, but a good relationship with the therapist does seem more important than anything else, and that factor being mostly independent from what modality the therapist uses may account for a large part of it.
Ultimately though, I think part of what my post is tries to do is point out that these different philosophies don't necessarily contradict each other, but rather are different lenses through which to view the problems the client has. When I get a client that responds super well to CBT, and then another client who doesn't but grabs IFS and runs with it, I don't think "well I guess these modalities are equally effective" or think that some kind of paradox is occurring, I just think that different maps are better for different people at navigating the territory, even if they're dealing with the same "problem."
I know it feels a bit like a cop-out, but honestly given how complex people are, and how different each problem can be even if it shares the same diagnosis, I would be pretty shocked if a single modality just blew all the others out of the water for every kind of problem that someone might face. Which isn't to say that they're all the same, either, just that guidelines for good therapy have to include more than just singling out specific modalities, but also identifying which ones might work best with each client.
↑ comment by Kaj_Sotala · 2020-10-13T15:47:18.517Z · LW(p) · GW(p)
3. Give 1 and 2 and the fact that therapy works for some reason and the fact that different types of therapeautic theories contradict each other, therapy must work not only because because it improves the patient's map of the territory, but also by another mechanism.
It felt to me like the overview of the therapeutic philosophies suggested a partial answer to this one: part of why different therapies contradict each other is that they describe different parts of the territory / have different mechanisms of action. E.g. if behaviorist therapy changes a person's conditioning and systematic therapy looks at the social system they are in, then there doesn't need to be a conflict: a person has their own individual conditioning, and that conditioning is also affected by the signals that they get from their social system. (Both are describing the same territory but emphasizing different aspects / levels of it, kind of analogous to physics and chemistry.)
comment by ioannes (ioannes_shade) · 2020-10-11T16:15:06.416Z · LW(p) · GW(p)
Reminds me a bit of this good thread by Qiaochu [LW · GW].
Replies from: DaystarEld↑ comment by DaystarEld · 2020-10-11T20:20:16.849Z · LW(p) · GW(p)
Yep, that was a great thread.
comment by Kaj_Sotala · 2020-10-13T16:05:39.038Z · LW(p) · GW(p)
"Chess Therapy" on your image made me go "what" so I looked it up:
Chess therapy is a form of psychotherapy that attempts to use chess games between the therapist and client or clients to form stronger connections between them towards a goal of confirmatory or alternate diagnosis and consequently, better healing. [...]
In psychoanalysis chess games are wish fulfillment, and that an important part of these wish fulfillment are the result of repressed desires—desires that can scare a person so much that their games may turn into a series of defeats. Chess games can be divided into wishful games, anxiety games, and punitive games.
I was about to say something like "okay, this is starting to sound silly even to me", but then I remembered that a linkpost to an article about self-sabotage in Magic: the Gathering [LW · GW] has been called one of the top most valuable things on LW [LW(p) · GW(p)], so I guess it's not that silly after all.
Replies from: DaystarEld↑ comment by DaystarEld · 2020-10-16T05:47:54.212Z · LW(p) · GW(p)
Yeah, I had (have?) high skepticism of its effectiveness too, and it's definitely not a modality I'd use myself, but then I remember that I have used board games in therapy before with younger clients, particularly families, and there's some surprising stuff that can come out by observing the way people play games :)
comment by roland · 2020-10-30T14:10:20.782Z · LW(p) · GW(p)
A good critical book on this topic is House of Cards by Robyn Dawes