Omicron Post #4
post by Zvi · 2021-12-06T17:00:01.470Z · LW · GW · 66 commentsContents
In Search of Bayesian Evidence The South African Study Denmark Anime NYC Boston SGTF in the UK Too Little, Too Late New coronavirus vaccine may eventually be needed for omicron variant, BioNTech CEO says South Africa Case Numbers Going Up Other Threads and News Probability Updates Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 35% → 65%. Chance that Omicron will displace Delta as most common strain: 85% → 95%. Chance that Omicron is importantly more virulent than Delta: 8% → 5%. Chance that Omicron is importantly less virulent than Delta: 35% → 50%. Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 80% → 95%. Will the CDC label Omicron a variant of high concern before 2022? 15% → 13%. Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 3% → 2.5%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30%. Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 3% → 3%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 12% → 17% (EDIT: Should have been at least 25%). Will Omicron be >1% of all cases by the end of the year? 70% → 93%. None 68 comments
Previous Omicron updates: #1, #2, #3. Last weekly non-Omicron update.
An introductory word: Thanks to Dominic Cummings, I have a lot of new readers, many from the United Kingdom, so I want to welcome all of you, and I hope at least some of you will stay when I turn to non-Covid questions. I am American so these posts focus on the United States, but I keep an eye elsewhere too, and mostly we’re all in this one together and the same conclusions apply. If you have good news sources and follows to keep a better eye on the UK or Europe for Covid purposes, or data sources anywhere I may not have noticed, I invite you to share them in the comments.
The constant refrain from all sources is ‘we will know more soon.’ Soon is continuously arriving. The new information we are learning hasn’t completely ruled out many possibilities, but it is broadly consistent with Omicron spreading fast and having a high degree of immune erosion/escape in terms of infection but not protection against severe disease.
Thus, to headline the core takeaways at the top, here’s broadly where I’m at as of now (probability estimates at the end, as before). I’d be surprised if any of these were wrong.
- Omicron spreads far more rapidly than Delta and is going to take over.
- This will come at us fast. Omicron will be the majority strain by the end of January. This happening by end of year is on the table.
- Omicron re-infects those who have already been sick, or breaks through to those who have been vaccinated, much more than Delta.
- Previous infection continues to protect against severe disease, hospitalization and death.
- Omicron doesn’t cause substantially more severe disease than Delta when it infects you, but we don’t know if it causes less severe disease yet, our evidence is ambiguous.
- Omicron cases on average are much more mild because there will be a much higher percentage of re-infections and breakthrough cases, which are highly protected against severe disease.
- The big peak is probably within a few months, so you don’t have time to wait for an Omicron-targeted shot. The current shots will still work against severe disease, so strongly consider getting vaccinated or boosted if you can.
- The best thing we can do to minimize the harm Omicron causes is to ramp up production of therapeutics, especially Paxlovid, as rapidly as possible, along with the necessary tests and other logistics to get the treatments to people in time to matter. The goal is mitigation at this point, not prevention.
- There is going to be a period early in 2022 when there are quite a lot of Omicron cases, such that it will be difficult to remain uninfected and it will likely be difficult to get any kind of medical treatment at a hospital. Be ready.
- Also be ready in case of lockdowns and other government restrictions, especially if you live in Europe where they’ve shown a willingness to use them. And if you’re immunocompromised or otherwise at high enough risk you need to be sure to not get Omicron, then the price of success is getting super paranoid soon and lock down hard, for at least several months.
In Search of Bayesian Evidence
How rapidly does Omicron spread? How far has it spread already?
Any given infection or reported group of infections, or even piece of data, is unlikely to be conclusive. But each one does have a likelihood ratio of how common it is to witness it in worlds where Omicron will spread extremely rapidly in the West, versus worlds where Omicron doesn’t do that. Similarly, they have ratios for how often how much of that comes from immune escape versus baseline infectiousness, how much protection remains against severe disease and death, and what the baseline severity of Omicron is.
Then we need to consider what we saw relative to what we expected to see. In general, no news is good news. If ‘nothing happens’ regarding Omicron, that continuously makes us less worried, whereas most news will make us more worried. Getting a constant string of bad news is expected, but how much of it did we get, how fast and how bad?
A lot of that depends on the extent to which various jurisdictions are looking for news. Taking a Trump-like approach of ‘if you didn’t run the tests you wouldn’t have that many cases’ does successfully postpone the bad news for at least a few days, and sometimes several weeks. All reports need to be adjusted for the amount of effort being put into finding data and generating reports.
The South African Study
Title and link: Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa.
This preprint was the first study about Omicron, and it doesn’t hold back. Author has a thread here.
Here’s the results section.
35,670 suspected reinfections were identified among 2,796,982 individuals with laboratory-confirmed SARS-CoV-2 who had a positive test result at least 90 days prior to 27 November 2021. The number of reinfections observed through the end of the third wave was consistent with the null model of no change in reinfection risk (approach 1).
Although increases in the hazard of primary infection were observed following the introduction of both the Beta and Delta variants, no corresponding increase was observed in the reinfection hazard (approach 2). Contrary to expectation, the estimated hazard ratio for reinfection versus primary infection was lower during waves driven by the Beta and Delta variants than for the first wave (relative hazard ratio for wave 2 versus wave 1: 0.75 (CI95: 0.59–0.97); for wave 3 versus wave 1: 0.71 (CI95: 0.56–0.92)).
In contrast, the recent spread of the Omicron variant has been associated with a decrease in the hazard coefficient for primary infection and an increase in reinfection hazard coefficient. The estimated hazard ratio for reinfection versus primary infection for the period from 1 November 2021 to 27 November 2021 versus wave 1 was 2.39 (CI95: 1.88–3.11).
Extending the period back to 1 November is going to decrease the magnitude of this effect somewhat, although case numbers in the earlier pre-mostly-Omicron period of November were low.
The study notes that it is studying reinfection risk rather than vaccine breakthrough risk, but the two should be highly correlated.
It looks like the study’s method was to match IDs of current infections to previous infections.
One worry is that this might fail to control for immunity declining over time since infection, beyond the 90-day window where reinfection risk is assumed to be zero. Given that they calculated no additional reinfection risk for Delta up through October, presumably this effect can’t be anything like big enough to explain the results.
Another note is this only counts infections that were detected on both occasions, which could have some interesting effects. Mostly I think this should undercount the rise in reinfections, because more of the control group were actually previously infected without knowing it, which is effectively a multiplier effect on the real odds ratio.
Here’s the key chart:
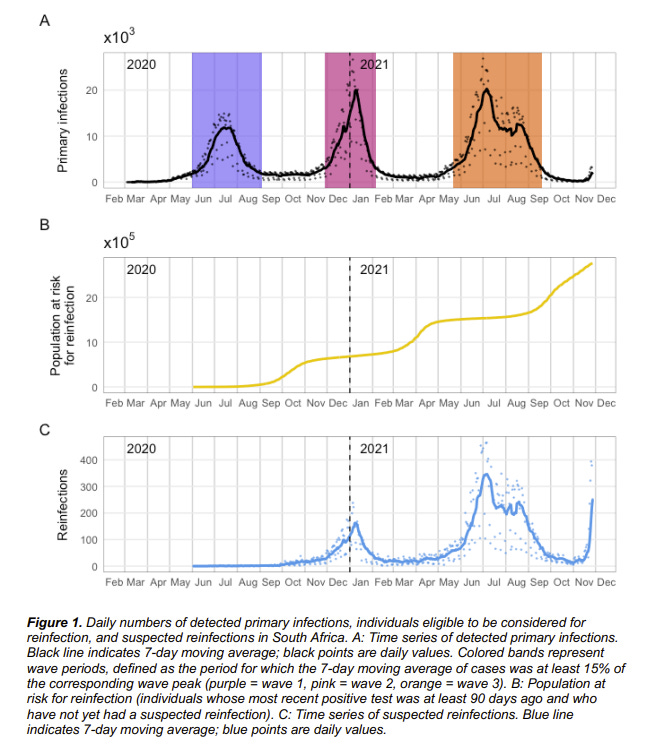
This is naked-eye obvious. The population at risk for (known) reinfection is roughly double what it was before, yet the ratio of reinfections to other infections is clearly much higher than that.
Also note that this finding rules out the possibility that most South Africans were already infected. If that was true, then being known to have been infected wouldn’t provide much additional protection.
They give us numbers that should be easy to work with, file under Huge If True:
The mean ratio of reinfection hazard to primary infection hazard decreased slightly with each subsequent wave, from 0.15 in wave 1 to 0.12 in wave 2 and 0.09 in wave 3.
The mean ratio of reinfection hazard to primary infection hazard for the period from 01 November 2021 to 27 November 2021 is 0.25.
Note that protection from an Omicron infection, for a future second Omicron infection, would probably still return to previous levels.
I am inclined to mostly believe this result, as it is broadly consistent with other findings.
Denmark
Link is to Washington Post report on Denmark’s huge jump in sequenced Omicron cases. Denmark does a lot of sequencing, so them finding a lot of cases first is a sign things are far along.
The number of confirmed cases in the country rose from 18 on Friday to 183 on Sunday, reflecting both the speed at which the variant has spreadand the sensitivityof Denmark’s virus surveillance system.
The northern European country is a leader in the sequencing of variants, acting as an early-warning system for the continent.
…
Health authorities in the country of 5.8 million perform more than 200,000 polymerase chain reaction, or PCR, tests per day — one of the highest rates of tests per capita in the world. Positive tests are submitted for special PCR tests that detect variants. For those that come back positive, scientists sequence the whole genome. Denmark sequences 25,000 strains per week, Lillebaek said.
…
Danish media reported that some of the infections were traced back to a concert in late November and a Christmas lunch involving 150 guests.
Britain also reported a sizable uptick in omicron cases: 86 new cases on Sunday, bringing the total number there to 246.
Attempts to trace Omicron cases are helpful, but in terms of knowing where we stand they can also corrupt the data. If Denmark was about as likely to catch an Omicron case of a given severity as a Delta case, and was sequencing all its 4300 tests a day (its 7-day average of positive tests), and got back 183 positive cases in a day, that would mean 4% of cases were already Omicron, and given what that would be saying about exponential growth, we’d expect to cross 50% within two weeks.
The question is, if we hadn’t been doing this extra tracking of Omicron cases, how many of the Omicron cases we did find would have been missed? If we don’t discount those, we’re going to get an overestimate, and of course Saturday could have been an outlier due to timing of data collection. If we catch every Omicron case, then we’d have to discount by the percentage of Delta cases that get missed, which is unknown, in addition to adjusting for exact timing. Even with a lot of testing I’d presume 50%+ of cases are missed, and plausibly 75%+. Denmark’s cumulative case rate is only 8.8% for the entire pandemic, so this ratio could be quite high.
What we do know is that up until a few days ago, they sequenced every positive test and found zero Omicron cases. Now they’ve suddenly found 183 in a single day, 4% of average daily positive tests.
Superspreader events are a thing, so it’s possible that this is luck, but there aren’t a bunch of other Denmark-like countries that also do all this sequencing, so there was only one ‘shot’ at this happening in this way. It’s a sign of very rapid spread.
Hopefully we will also track outcomes from the group, to help us learn about severity. The numbers are starting to get big enough that they’ll tell us something, but that still requires time for cases to develop.
Anime NYC
The Omicron timeline needs to be moved up substantially, because the case that we found in Minnesota was a case of community spread, probably at a large Anime convention in NYC, and on November 19-21, which predates the identification of Omicron.

The case was not only vaccinated but boosted, and a majority of the friend group later tested positive. Things are escalating quickly, and we’re not making that much effort to find cases. This was identified as Omicron as part of a random sampling rather than any reason to suspect the case, which is also worrisome, and there was still an 8-day delay involved. Ouch.
Our awful mayor issued this statement afterwards, along with others who urged those in attendance to get tested.
But look at the timing. They’d all already been infected over a week ago. What’s the point?
Boston
This is a graph of the amount of Covid found in the wastewater in Boston. If you have links to similar other measurements taken regularly, share them in the comments.
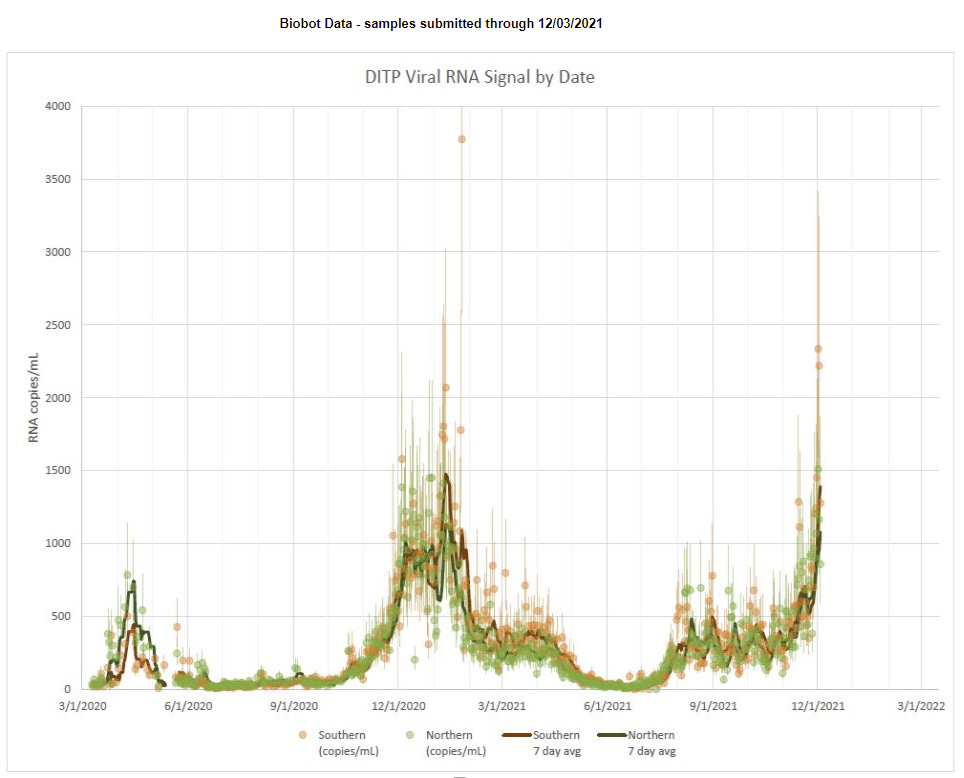
That spike on the right has two of the three highest single-day measurements, and they were the last two days of data reported. This can’t represent Delta cases alone unless it’s a data error, because the rise is too rapid given what we know about conditions. If it’s Omicron and the measurements are what they superficially look like, it means Omicron is already primary in Boston, and there’s a huge spike in infections already, that hasn’t been matched with a surge in hospitalizations or positive tests.
There are other outlier measurements on the graph, so probably these are outlier measurements. But if they hold up over the next few days, then what would that mean?
If they hold up and there isn’t a wave of new hospitalizations quickly, then this is the best of all possible worlds. Omicron would be spreading like wildfire, but be much milder than previous waves. We’d be able to get through it quickly, and have no realistic way to prevent it, so all we could do would be to shield the vulnerable to the extent we could, use what treatments we have that we can get to be legal, and come out the other side.
If they hold up and then the hospitalizations follow then things are quite bad, it’s hitting us now and we’re in a crisis situation. There will be pressure to do very foolish things to try and stop something that will be utterly impossible to stop, and Paxlovid will arrive too late to make much difference.
If they don’t hold up, that’s mostly what I expect. Either it’s bad or weird data, or Omicron somehow puts a ton more virus into the wastewater, and then there’s nothing to see here. That’s what I mostly expect, but note that the measurement happened in both the north and south sections, which didn’t happen on the previous big fluke measurement.
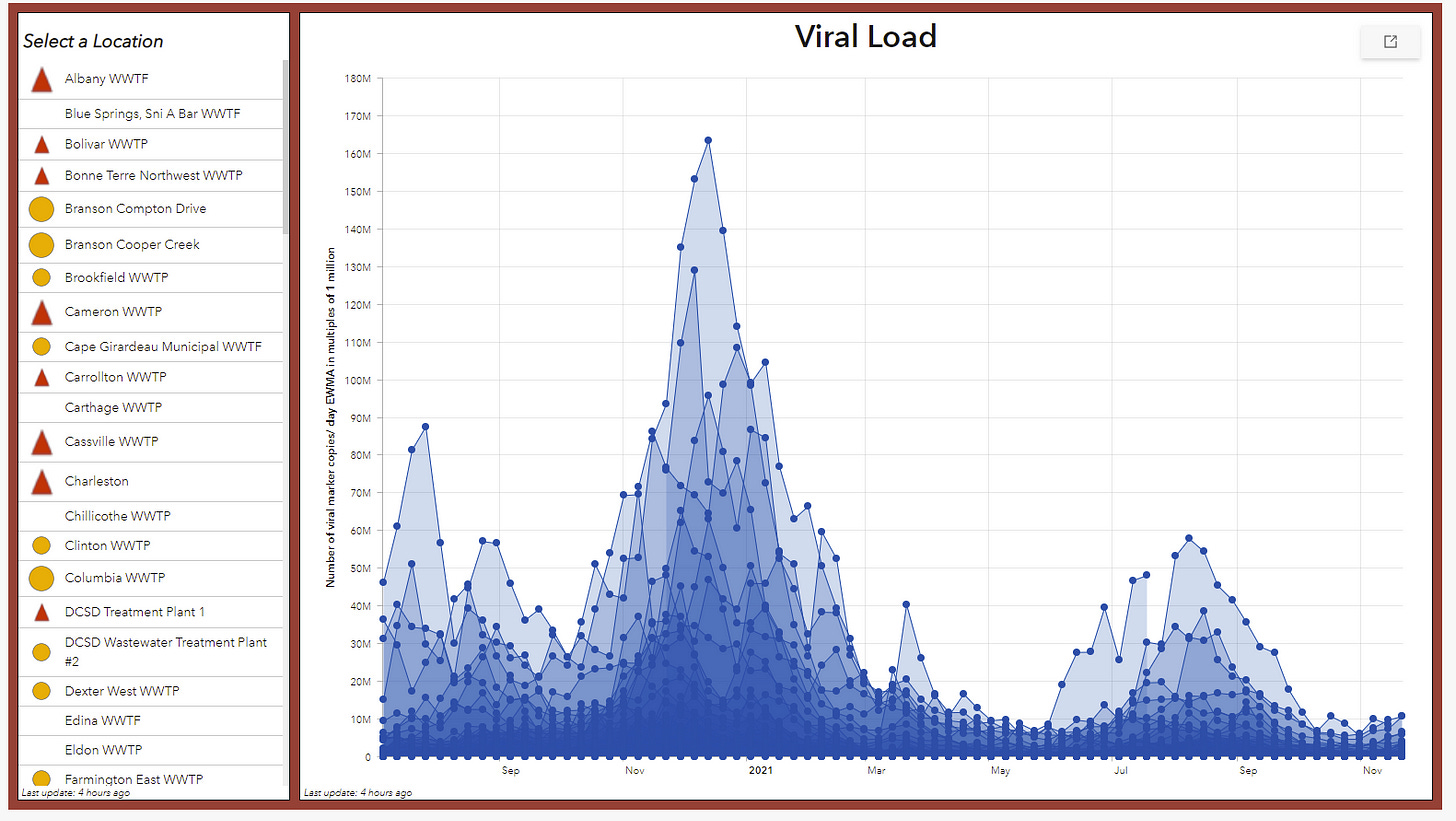
Here’s a graph in Missouri that doesn’t yet show a similar spike, but is updated less often and is from a less internationally connected area. As you’d expect, no spike.
There’s also this Dutch source, which shows no spike yet.
Unfortunately that was the only other ones I found so far. There’s implications in the next section’s threads that such data is available for the UK but I’m not sure where to find it.
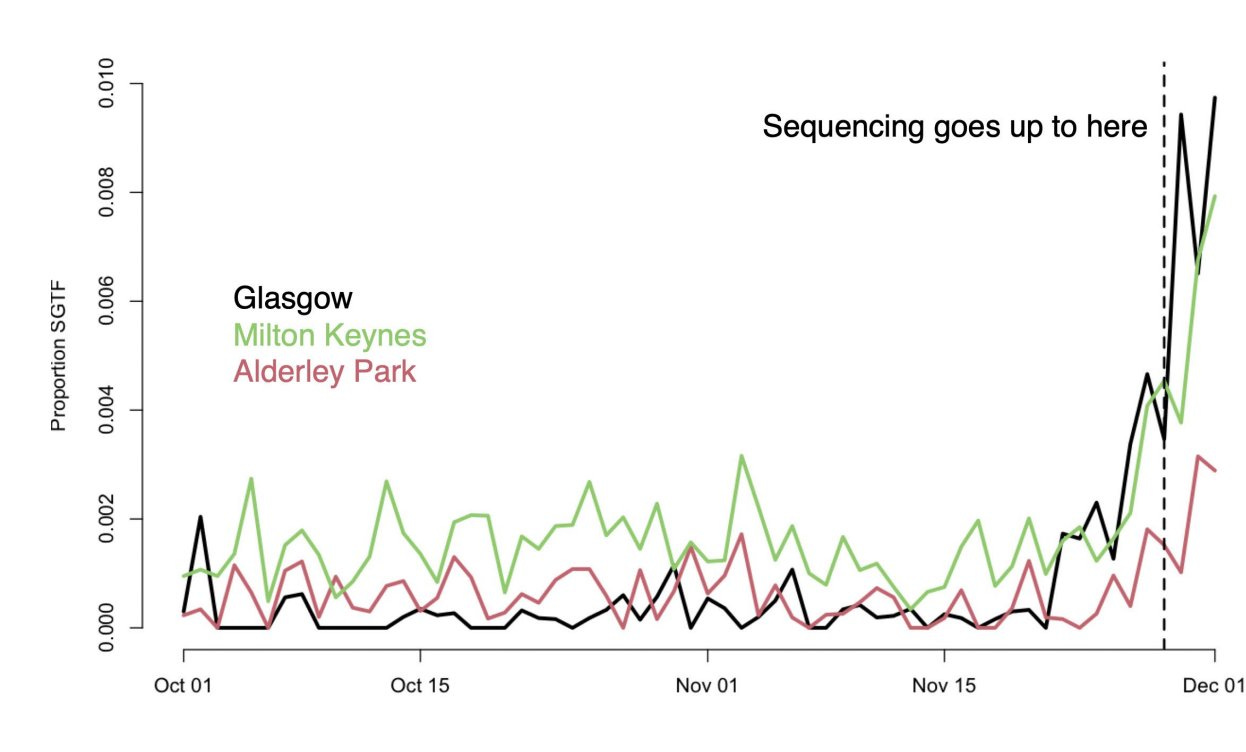
SGTF in the UK
Oops. As of December 3.
Too Little, Too Late
Scott Gottlieb warns us not to act prematurely, despite it already being too late:
Noting that companies, including Pfizer, were doing so, Gottlieb said, “This is going to be a really critical decision because what we’ve seen in the past, for example, when we engineered a vaccine to specifically target 1351, the old South African variant, was that vaccine worked well or appeared to work well against 1351 but didn’t appear to provide as good coverage against all the other variants.”
“And there’s reason to believe that as you develop vaccines that are very specific to some of these new variants, they may not work as well against the full complement of different variants that we’ve seen. So you wanted to try to stick with the ancestral strain, the Wuhan strain, in the vaccine, I think, as long as possible,” Gottlieb continued.
I don’t want to pick on Gottlieb because he’s better than most, but this is emblematic of a system that never acts in time when it matters. Given the logistical timelines involved, even if we made a full best effort starting today, we’d largely be too late getting the new Omicron vaccines to those who need them. Waiting until Omicron is already dominant or far enough on its way to make it the kind of obvious being looked for here is a way for exponential growth to laugh in your face every single time.
Exponential growth doesn’t permit one the luxury of being exactly on time. Either you’re too early or you’re too late. You either move now and have some chance to do some good, or you’re way too late.
Here’s another Washington Post headline showing the extent to which we will get there too late and with too little.
New coronavirus vaccine may eventually be needed for omicron variant, BioNTech CEO says
…
“I believe, in principle, we will at a certain time point need a new vaccine against this new variant. The question is how urgent this needs to be available,” CEO Ugur Sahin told a conference hosted by Reuters.
He also said the current vaccine could be adapted “relatively quickly” if needed to combat the omicron variant, but cautioned that more research was still required.
If that’s the attitude of the CEO of BioNTech, that should both put to bed any rumors that the vaccine companies are trying to trick us into taking extra vaccines to make them more money (which was already absurd, and no doubt will never be put to bed no matter the evidence, but shrug) and also put to bed the hopes that the new doses could arrive in time. This essentially indicates that the serious push will only begin after Omicron is a large share of cases and then it will be far, far too late.
Similarly, here’s the head of the CDC saying true things that complete miss the point and the urgency.
“We know we have several dozen cases and we’re following them closely. And we are every day hearing about more and more probable cases so that number is likely to rise,” Walensky said on “This Week.”
If something is certain, it is also probable.
“We have about 90 to 100,000 cases a day right now in the United States, and 99.9% of them are the delta variant,” Walensky said.
This is probably true, although I think there’s a non-trivial chance Omicron is already over 0.1% of cases, but it won’t stay true for long and isn’t all that relevant.
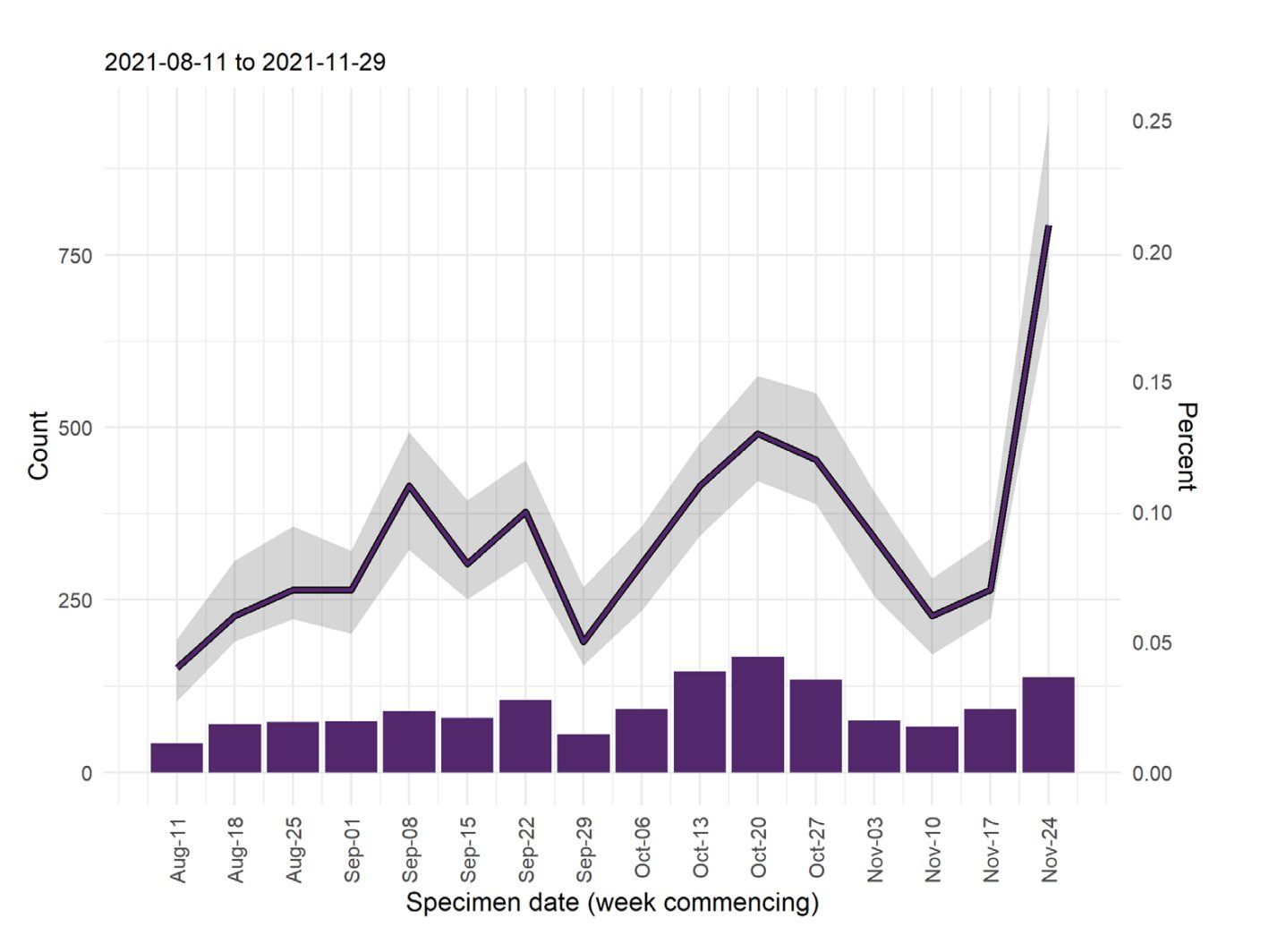
South Africa
The person linking to this thought it was bad news, but given the rate at which cases are increasing, it looks to me like good news. Not easy to interpret, but the hospitalization rate per infection is what matters here. Note also that positive test rate is now >20%, which means a higher percentage of cases are being missed than before.
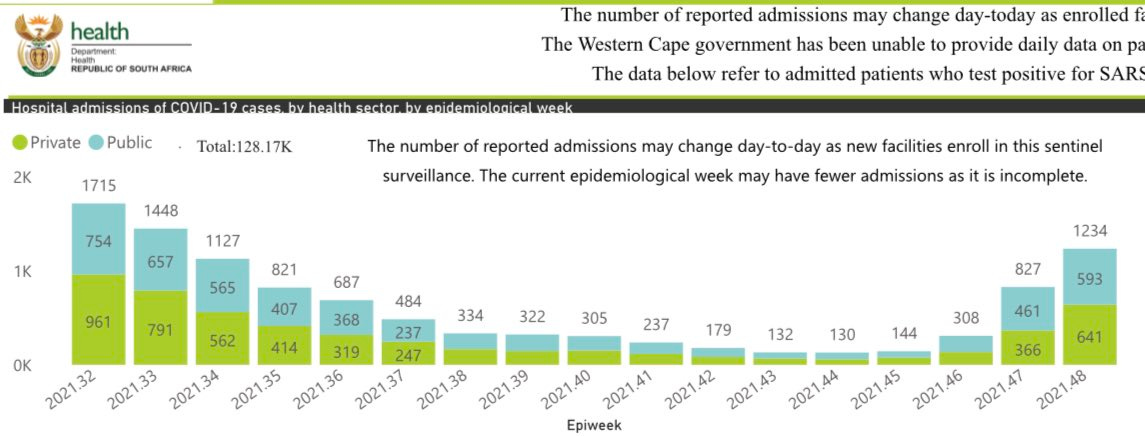
Here’s some South African data by province:
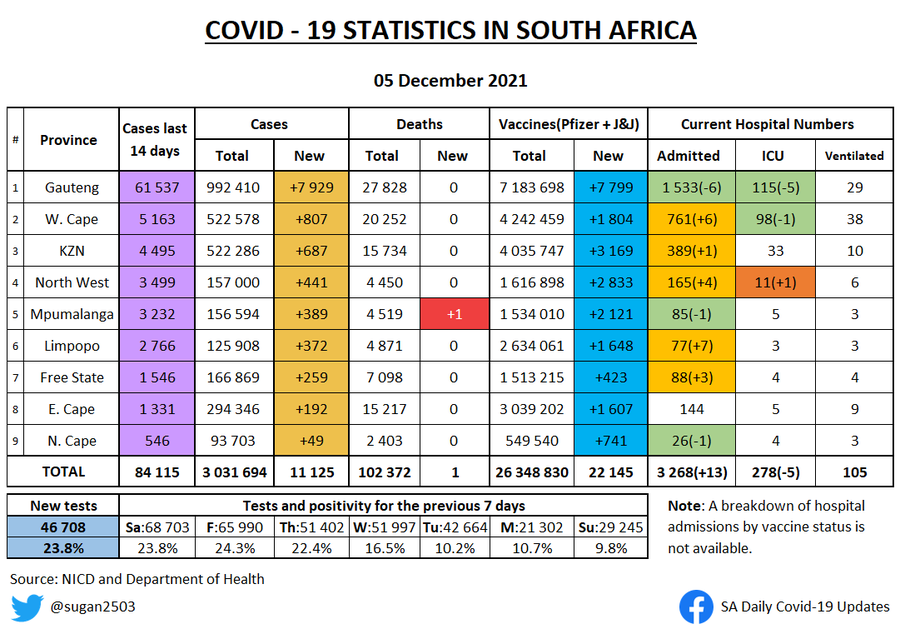
If I’m reading both charts correctly, the ratio here seems quite good, actually.
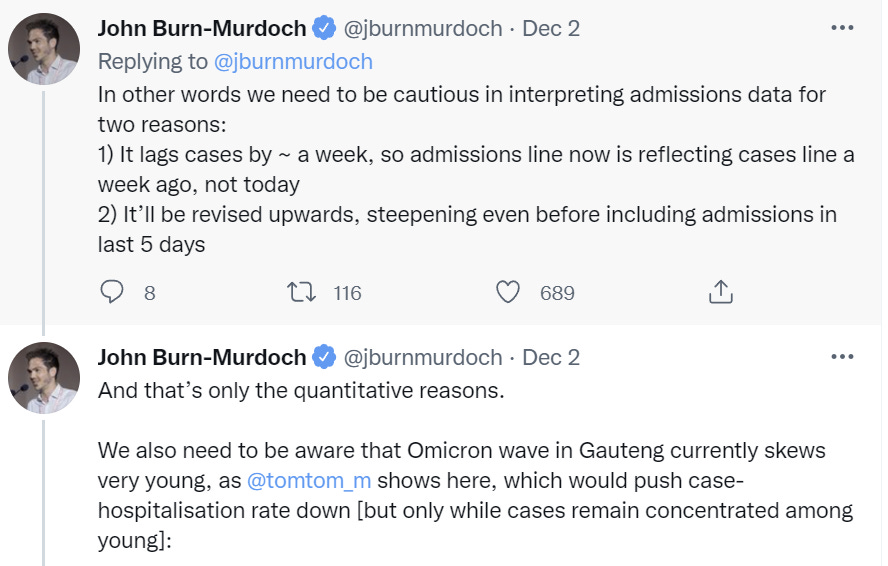
The December 2 version of the summary graph from Gauteng.
The thread that was in gives some caveats on the hospital numbers, they get revised upwards later and lag cases, but still.
Then here’s the chart from December 4.
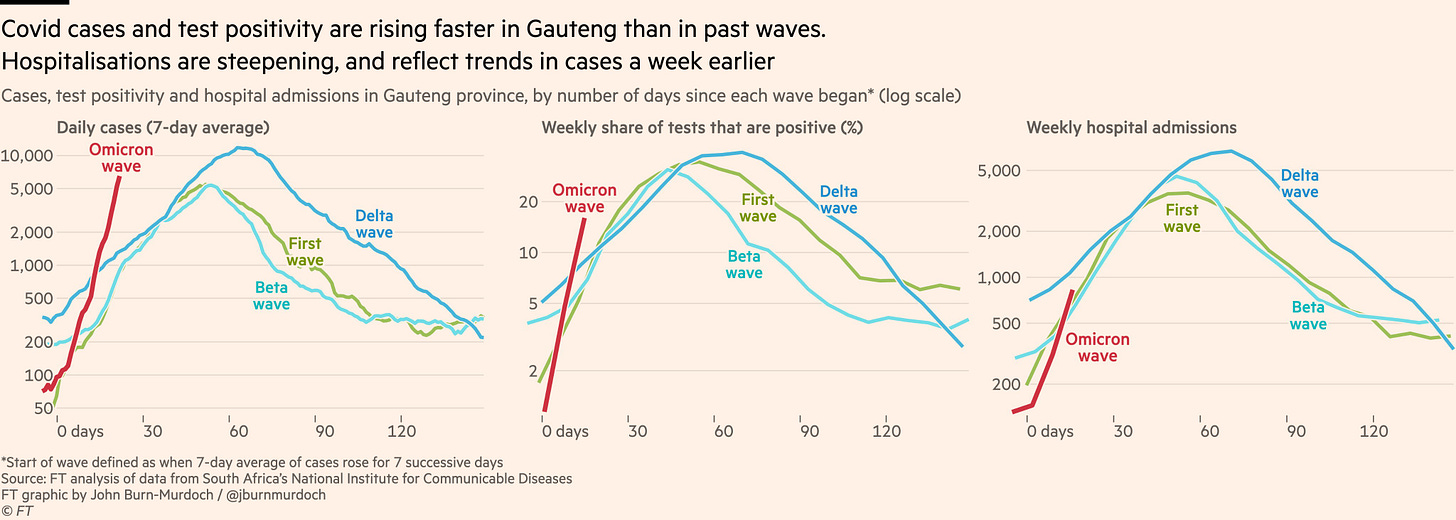
Preliminarily it looks good, but I still don’t feel we can conclude anything.
Here is a summary of patient profiles from Gauteng. In general, the patients are healthier than one would expect, even accounting for age. I found this especially interesting:
In summary, the first impression on examination of the 166 patients admitted since the Omicron variant made an appearance, together with the snapshot of the clinical profile of 42 patients currently in the COVID wards at the SBAH/TDH complex, is that the majority of hospital admissions are for diagnoses unrelated to COVID-19. The SARS-CoV-2 positivity is an incidental finding in these patients and is largely driven by hospital policy requiring testing of all patients requiring admission to the hospital.
Think about what this implies. If a majority of the cases that have Covid-19 were admitted to the hospital for unrelated reasons, then either Covid is somehow causing all these ‘unrelated reasons’ without making the patients sick with Covid in an obvious way, or the chance of hospitalization in the window when you have Covid less than doubles. You’re more likely to be admitted to the hospital and happen to have Covid, then for Covid to send you to the hospital.
If that’s true, then that seems like a very mild disease indeed. Anyone else want to take a shot at interpreting the data here?
Case Numbers Going Up
There was a superspreader event in Oslo.
OSLO (AFP) – Norway introduced new anti-Covid measures in greater Oslo on Thursday (Dec 2) after a suspected cluster of Omicron cases emerged among dozens of vaccinated people.
Face masks will be mandatory in public transport, shopping centers, shops and taxis when social distancing is not possible.
People will have to work from home if possible and the number allowed to gather at private indoor events will be limited to 100, the government said.
The announcement came after the Omicron variant was detected in at least one of “50 to 60” people who tested positive for Covid-19 after a Christmas dinner in Oslo last week.
That represents about half of the 120 people – all vaccinated – who attended the event organized by solar energy producer Scatec.
Superspreader events are outliers by definition but that’s almost half of the people attending all of whom were vaccinated. I do not believe that is a thing that could have plausibly happened under Delta. They haven’t officially confirmed these were all Omicron cases yet, but it seems unlikely they aren’t mostly or entirely Omicron.
The response of tightening restrictions in the area seems unlikely to accomplish much.
Other Threads and News
Noah Smith’s second summary thread. I intentionally read this last. It’s solid, but doesn’t contain much additional information.
Thread illustrating the range of possible properties of Omicron, and how its infectiousness interacts with its immune escape properties. Correctly suggests that any efforts need to start now to have any chance of arriving in time. Doesn’t think Omicron is likely to be less infectious, but that seems like it was mostly priors.
Jose Caballero thread from December 2.
Poll claiming that Americans are quite open to additional measures against Omicron.
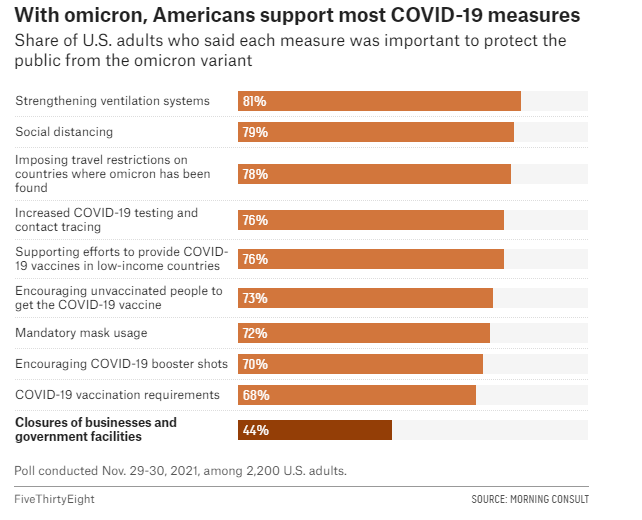
Note how crazy it is that there are 68% of people support mandatory vaccination but only 70% (2% more!) people support encouraging booster shots. There are almost no people with the ‘encourage people to do useful things but don’t force them to do those things’ position. Sigh.
Bad news on monoclonal antibodies (WSJ), but isn’t surprising given what else we know.
An attempt to synthesize what we know while incorporating Metaculus predictions, from December 2. Included for completeness, but nothing new or surprising.
Probability Updates
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 35% → 65%.
Note that I am interpreting this as ‘in practice in the United States of America,’ or in Europe, rather than the transmission advantage in an immunologically naïve person.
We have the growth in cases in Denmark and around the world, the paper from South Africa, the continued case growth in South Africa, the wastewater in Boston (even if I’m not sure if this is ‘real’ yet) and the superspreader events in Oslo and at Anime NY. We have cases being found within a few days, in multiples, from nothing, across most countries that checks for cases.
After a certain number of exponential curves, it’s hard to deny what you are looking at. I’m not willing to go super high on this yet because 100% is a very high threshold, and variants often have large advantages when they are first spreading that don’t carry over to later on, but this seems more likely than that.
Chance that Omicron will displace Delta as most common strain: 85% → 95%.
With the extent of immune escape we’ve seen and the rapid growth in cases, I don’t see a plausible path to this not happening. The likelihood ratios this week were very high, and model or systematic error is the reason I’m not going higher than this.
Chance that Omicron is importantly more virulent than Delta: 8% → 5%.
Chance that Omicron is importantly less virulent than Delta: 35% → 50%.
If Omicron were more virulent than Delta that would make our observations so far very unlikely. It’s not impossible that this is the case and the huge number of young people infected and number of breakthrough infections and reinfections are disguising it, but this becomes less likely over time.
With respect to being less virulent than Delta, there’s a bunch of suggestive findings that have cases or implied cases rising without a rise in hospitalization. I am increasingly hopeful that we did indeed get lucky on this and anyone saying ‘no evidence’ here has very little leg to stand on.
However, I still think this is only a coin flip, because the data we have is too confounded by too many factors, as discussed above.
Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 80% → 95%.
Will the CDC label Omicron a variant of high concern before 2022? 15% → 13%.
The data on immune erosion seems very clear. There’s enough uncertainty it’s not fully over (and I am moving fast enough that I admit I’m not being all that principled or accurate in my various 5% chances here in terms of exact percentage) but I don’t see how we get the data we’re getting without this being the case.
As for the label of high concern, that’s a question of how and how fast the CDC works and I grow increasingly skeptical that they will ever do anything with speed, and the prediction market on this has been up for longer as the deadline grows closer.
Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 3% → 2.5%.
The data doesn’t make sense if this is false but I don’t want to get too confident too quickly.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 30% → 30%.
It looks like it will take three months to complete the whole process and get the new vaccine formulations approved, at which point boosters will become available, and by the time any given person can in practice get a shot, it will likely be more than 6 months after their last shot unless they delayed on the booster quite a bit, which likely means they’re not high priority. So my guess is in practice this won’t happen, but the whole thing is odd and ambiguous. I should likely formulate a more precise question that better answers what we care about.
Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 3% → 3%.
No new information.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 12% → 17% (EDIT: Should have been at least 25%).
I’m going back up on this based on a higher certainty that Omicron is the real deal, and the higher chance it’s a very fast version of the real deal that is likely to peak quite high and overwhelm the hospitals temporarily. If that happens, there’s going to be a lot of pressure for extreme measures. What’s keeping this from rising more is the possibility the cases will remain mild.
EDIT: Commenters pointed out that while this seemed like a big adjustment, it definitely wasn't enough and the other updates implied a bigger change, to at least 25%, depending on the exact definition and how many components need to apply.
Will Omicron be >1% of all cases by the end of the year? 70% → 93%.
The market on this is trading too low. There’s very little chance this does not happen given the new timelines. There’s still some uncertainty here, but it’s declining rapidly, and it’s mostly model uncertainty.
66 comments
Comments sorted by top scores.
comment by Dave Orr (dave-orr) · 2021-12-06T18:17:23.251Z · LW(p) · GW(p)
Thanks for all the work you put in on these incredibly informative posts. This is, hands down, the best source of analysis I've found for all things COVID.
Replies from: lsusrcomment by Bucky · 2021-12-06T20:54:58.725Z · LW(p) · GW(p)
These quick updates on omicron are great - I’m super grateful I don’t have to wait a week between updates!
One question I had:
There is going to be a period early in 2022 when there are quite a lot of Omicron cases, such that it will be difficult to remain uninfected and it will likely be difficult to get any kind of medical treatment at a hospital. Be ready.
vs
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 12% → 17%.
These two things seem fairly similar - I wouldn’t expect it to take much to go from [difficult to get treatment] to [widely overwhelmed]. At which point I’d expect large lockdowns although I know the US is more resistant to this. Maybe the difference is bigger than I’m picturing.
Could you expand on your model here? In terms of actions I should be taking this seems to be the most important prediction.
Replies from: Zvi↑ comment by Zvi · 2021-12-06T21:23:47.931Z · LW(p) · GW(p)
My model is that 'hospitals are at capacity and under stress, and turn you away a lot' is pretty much baked in, but 'this turns into a crisis where we have people dying in the corridors and emergency conditions imposed' as a compound statement is a lot less likely. Still, I agree that 17% was too low, and I should have been more like 30%.
comment by arunto · 2021-12-06T19:30:17.644Z · LW(p) · GW(p)
Maybe I am extrapolating too much from the hospital situation here in parts of Europe (due to Delta's seasonality, not yet to Omicron) but I think the probability of widely overwhelmed hospitals is still too low with 17%, taken together with your other stated probabilities:
a) 50% Omicron not importantly less virulent than Delta (rephrased statement)
b) 95% Omicron most common strain
c) 65% Omicron with a transmission advantage of more than 100%
If we take that, and in addition,
d) Low vaccination rates in many US states outside of New England (NPR vaccination tracker).
then I would think about 30% is more likely, because the chance of not vaccine protected persons being infected with a virus not importantly less virulent should massively increase given your probabilities. (Actually maybe more than 30%, but the possibility of fast availability of treatment options, e.g. Paxlovid, has to be taken into account).
Replies from: Zvi, cistrane↑ comment by Zvi · 2021-12-06T21:22:12.372Z · LW(p) · GW(p)
Yeah, that's fair. I think what's going on is that I'm asking a compound question, and 'overwhelmed hospitals but we don't respond with severe restrictions' would be a no, but also I didn't update this enough. The 35->65 update directly should raise this and I should have been at 25-30.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-07T02:43:45.256Z · LW(p) · GW(p)
Oof, yeah, that sounds like playing to an inside straight. You're braver than I.
↑ comment by cistrane · 2021-12-10T19:15:22.060Z · LW(p) · GW(p)
In US States with low vaccination rates, what is the estimated amount of people who already recovered from earlier covid strains? If it is higher than in South Africa, most of these recovered unvaccinated will have protection which is similar to vaccinated but without a booster.
comment by Pattern · 2021-12-06T22:06:32.966Z · LW(p) · GW(p)
Note how crazy it is that there are 68% of people support mandatory vaccination but only 70% (2% more!) people support encouraging booster shots. There are almost no people with the ‘encourage people to do useful things but don’t force them to do those things’ position. Sigh.
Maybe it's been concluded that 'encouraging' will lead to 'it is mandatory'. It could also be that the two aren't sufficiently distinct to survey takers.
Maybe a more specific proposal/question will get different results.
Replies from: JenniferRM, gabriel-holmes↑ comment by JenniferRM · 2021-12-07T08:55:44.020Z · LW(p) · GW(p)
I think I'm in that 2% slice, and my feeling is that this position arises from:
- Having a moderately coherent and relatively rare theory of "benevolent government and the valid use of state power" that focuses on public goods and equilibria and subsidiarity and so on.
- Having a relatively rare belief that vaccinated people seem much more likely to get asymptomatically infected and to have lower mortality BUT also noting that vaccines do NOT prevent infectiousness and probably cannot push R0 below 1.0.
Thus, I consider covid vaccines primarily a private good that selfishly helps the person who gets the vaccine while turning them into a walking death machine to the unvaccinated.
They get a better outcome from infection (probably, assuming the (likely larger) side effects of boosters aren't worse than the (likely more mild) version of the disease, etc, etc) but such vaccine takers DO NOT protect their neighbor's neighbor's neighbor's neighbor's neighbor's neighbor from "risk of covid at all"...
...and thus my theory of government says that a benevolent government will not force people into medical procedures of this sort.
A competently benevolent government wouldn't mandate a "probably merely selfishly good thing" in a blanket way, that prevents individuals from opting out based on private/local/particular reasoning (such that it might NOT be selfishly beneficial for some SPECIFIC individuals and where for those individuals the policy amounts to some horrific "government hurts you and violates your body autonomy for no reason at all" bullshit).
Like abortion should be legal and rare, I think? Because body autonomy! The argument against abortion is that the fetus also has a body, and should (perhaps) be protected from infanticide in a way that outweighs the question of the body autonomy of the fetus's mother. But a vaccine mandate for a vaccine that only selfishly benefits the vaccinated person, without much reducing infectiousness, is a violation of medical body autonomy with even less of a compensating possible-other-life-saved. Vaccine mandates (for vaccines that don't push R0 lower than 1) are probably worse than outlawing abortion, from the perspective of moral and legal principles that seem pretty coherent, at least to me.
I think many many many people are gripped by a delusion that vaccines drop R0 enough that with high enough vaccination rates covid will be eradicated and life will go back to normal.
(Maybe they are right? But I think they are wrong. I think R0 doesn't go down with higher vaccinations enough to matter for the central binary question.)
Then, slightly separately, a lot of people think that the daddy/government can make them do whatever it wants so long as daddy/government verbally says "this is for your own good" even if that's a lie about what is objectively good for some individual people.
A key point here is that my theory of government says that IF there is a real public good here, like an ability to pass a law, throw some people in jail for violating the law, and then having a phase change in the public sphere leading to a dramatically better life for essentially everyone else such that the whole thing is a huge Kaldor-Hicks improvement... THEN that would be a just use of government coercion.
This general formula potentially explains why stealing gets you thrown in jail. Also why cars speeding fast enough in the wrong place gets you thrown in jail. You want "a world where bikes can be left in front yards and kids can safely cross the streets" and throwing people who break these equilibria in jail protects the equilibria.
I don't see how "infecting people with a lab created disease" is vastly different from speeding or stealing? Harm is harm. Negligence (or full on mens rea) is negligence (or full on mens rea).
If vaccines prevented transmission enough to matter in general, then vaccines COULD be mandated. But the decision here should trigger (or not) on a "per vaccine" basis that takes into account the effects on R0.
Then, sociologically, most people haven't even heard of Pareto efficiency (much less Kaldor-Hicks) and most people think these vaccines are a public good that will eventually end the nightmare.
So I guess... you could test my "theory of opinion" by explaining "classical liberal political economy" and "bleak viral epidemiology" to lots of people, and then, as a post test, see if the 2% slice of the population grows to 3% or 4% maybe?
If lots of people learn these two things, and lots of people start opposing mandates for the current set of vaccines, that would confirm my theory. I guess you could also falsify my theory if anti-mandate sentiment rose (somehow?) without any corresponding cause related to a big educational program around "libertarian epidemiology"?
I have heard of Kaldor-Hicks efficiency AND ALSO I think the nightmare will "stop" only when the virus evolves to be enough-less-nightmarish that it seems no worse than the flu.
But note! My model is that the virus is in charge. And "covid" will in some sense happen forever, and the situation we're in right now is plausibly the beginning of the new normal that will never really stop.
Hopefully milder and and milder variants evolve as covid learns to stop "playing with its food", and things sorta/eventually become "over" in the sense that the deaths and disabilities fall to background levels of biosadness? But that's the only realistic hope left?
And I wish I was more hopeful, but I'm focusing on "what's probably true" instead of "what's comforting" :-/
I guess hypothetically in 2022 or 2024 politicians could run on (and win with?) a proposal to "totally and completely revamp all of the medical industry from top to bottom in a dramatic enough way that actual disease eradication is possible, such as by deleting the FDA, and quickly constructing a public disease testing framework with new better tests under a new regulatory system, that quickly tests everyone who wants a test every single day they are willing to voluntarily spit into a cup, and then do automated tracing with data science over the voluntary test data, and then impose involuntary quarantine on the infectious in judiciously limited but adequate ways, and just generally make covid stop existing in <NationalRegion> from a big push, and then also have adequate testing be required to get in and out of the country at every border and port, and so on with every coherent and sane step that, altogether, would make covid (and in fact ALL infectious disease in the long run) simply stop being a problem in any part of the world with governmental biocompetence."
But this will also probably not happen because we live in the real world, which is not a world with good politicians or wise voters or competently benevolent cultural elites.
We are bioincompetent. We could have eradicated syphilis for example, and we chose not to. Syphilis mostly affects black communities, and the US medical system doesn't competently care about black communities. We suck. Covid is our due, based on our specific failures. Covid is our nemesis.
The view from the 2% slice says: lean back, hunker down, and enjoy the ride. Its gonna suck, but at least, if you survive (and assuming the singularity doesn't happen, and grandkids are still a thing 40 years from now, etc, etc, etc) then you can come out of it with a story about generalized civilizational inadequacy to tell your grandkids.
Replies from: Daniel V↑ comment by Daniel V · 2021-12-08T16:07:39.241Z · LW(p) · GW(p)
Your POV really turns on (emphasis added):
Having a relatively rare belief that vaccinated people seem much more likely to get asymptomatically infected and to have lower mortality BUT also noting that vaccines do NOT prevent infectiousness and probably cannot push R0 below 1.0.
Much more likely than what? It would seem the relative comparison you want to make would be vs. the unvaccinated, but that's obviously false (and that's the important part). It's true they are more likely to be asymptomatically vs. symptomatically infected (yay mild COVID), but so what? Most of the work is done on any infection at all, e.g. (making up numbers but illustrating the point):
P(infected | unvaccinated) = .50, P(asymptomatic | infected for unvaccinated) = .50, and then assume that symptomatic people are less likely to transmit the disease than asymptomatic people because they know to quarantine thanks to the symptoms. So that's a 25% chance of getting asymptomatically infected feeding into a decision generating a negative externality.
P(infected | vaccinated) = .05, P(asymptomatic | infected for vaccinated) = 1.0, let's assume there are no symptomatic cases of infections among the vaccinated (hahaha), that's a 5% chance of getting asymptomatically infected feeding in. Again, most of the work is done on any infection at all, so having a higher chance of symptomatic (vs. asymptomatic) infection doesn't really matter (at the level of vaccine effectiveness and rate of asymptomatic infection we've seen).
Do vaccines prevent infectiousness? I remember seeing CDC data over the summer about how symptomatic vaccinateds are as infectious (in viral load) as symptomatic unvaccinateds, so that's conditional on showing symptoms. But let's assume asymptomatics in each group are also equally infectious - then we can still favor vaccines because, see above, most of the work is done on any infection at all.
To conclude, I think it's extremely clear that your (2) is wrong. There is public good value to vaccination.
Replies from: JenniferRM, cistrane↑ comment by JenniferRM · 2021-12-09T01:14:06.961Z · LW(p) · GW(p)
Thank you for this high quality response! The numbers were helpful and I had to stop and grind out some of the math and parse your sentences carefully.
assume that symptomatic people are less likely to transmit the disease than asymptomatic people because they know to quarantine thanks to the symptoms.
Making this part of the model more quantitative might reveal a crux?
I think we agree here directionally (symptomatic people change behavior in a way that has pro-social results, exposing fewer people "out in the world") but if the effect was very large (like if the average asymptomatic person infected a mean of 30 people and the average symptomatic person only infected 1.1 people) then I think it might overwhelm other parts of a full model, even with the numbers you specified (which I will get to below).
(Empirical Digression:
This meta-analysis suggests that on the order of a half to a third of all infections occur not "out in the world" but specifically in a medical context... where "worse symptoms" might tend to evolve in order to cause infected people to go to clinics where they could infect a large portion of the people who ever get infected with covid.
This other study suggested that "Brigham and Women’s Hospital" in Boston had a much much lower rate of nosocomial covid, so covid's evolutionary incentives under endemic conditions might be regionally heterogeneous?
Under an institutional heterogeneity model... it might be pro-socially wise to isolate any region with normally bad hospitals until these breeding grounds of infectious mortality are closed or repaired to adequacy. Obviously we are not wise, however, so this is unlikely to happen even if it was a net good for sure. Also, the model might be false, and it is certainly controversial, so I do not advocate this directly right now, based on current credence levels.)
In terms of your proposed model I think you didn't specify how many more people the average asymptomatic covid carrier might infect but you did give these:
P(infected | unvaccinated) = .50
P(infected | vaccinated) = .05
P(asymptomatic | infected & NOT-vaccinated) = .50
P(asymptomatic | infected & vaccinated) = 1.0
A common problem in bayesian modeling is to figure out what your "event space" actually contains. In a nutshell: what are you counting? "Mere counting" can sometimes turn out to be hard...
I'm not sure if "infected" for you means "infected in a specific single exposure event during a controlled challenge trial that is a decent proxy for a normal exposure event" or if it means some sort of lifetime all-in summary statistic closer to incidence or prevalence or a time and/or space bounded attack rate.
I mostly focus on these macroscale summary statistics, and so my model is that the attack rate for the period from 2018 to 2025, assuming endemic covid and no eradication and so on, might be close to 100% and it might even be higher than 100% if the numerator is "periods of infectiousness by a single person with covid in a region" (so asymptomatic re-infections cause +1 to the numerator) and the denominator is "total people in that region".
Like in the worst possible world, covid evolves to higher and higher mortality, such that all humans are either dying or else vaccinated against the variant that came out in the last 12 months (and also everyone "healthy" is semi-chronically infected in a way that is non-fatal after vaccination), always, in general, like some kind of Paolo Bacigalupi story?
And I get it. If the world is on fire and vaccination protects you from being hurt by being on fire... I'd get the vaccine too. I did get the vaccine, even knowing it was might only be selfishly beneficial. At this point: any port in a storm, you know?
So for me, thinking of "P(infected)" as a summary statistic for a person in a region with endemic covid... that shit is probably going to be very high even for the vaccinated. I think?
Concretely then, I assert P(infected | vaccinated) >> 5% (for an understanding of the relevant event space where this number applies over a long period of time, like any five year period during which covid is endemic and still evolving).
Maybe you know otherwise, and this is a crux?
But I think I'm right, because I think that is basically what it means for covid to be endemic forever. Like... the only people who won't get infected under endemic conditions (maybe over and over?) will be lifetime shut-ins?
Measles used to have an insanely high R0 and a 1% mortality and we nearly eradicated it back when our medical system was competent, so the the niche is kind of empty?
Before the competent near eradication of measles everyone got "the 1% fatal, high R0, disease", and if you lived then you lived, and that's why our genomes are full of disease-protecting alleles. Now the global bio-techno-governing-medical system is either evil or incompetent or both... so maybe there is an open niche? Maybe the human genome will eventually get new alleles for this?
Epistemically (if you with agree my modeling ideas and event space choice) it would be convenient because it might mean that we can just look up the attack rate overall (and maybe look up the relative R0 contributions) and "simply know" the same thing :-)
Personally, if we're granting that this thing is politically impossible to eradicate, I think the right thing to focus on might be modulating the evolution of covid to be "slow and towards lower mortality".
(If we can't eradicate, I suspect this more subtle form of influence over covid is probably also beyond our politico-economic capacities and we will just experience whatever nature does to us, like savages subject to the whims of the lesser gods.)
I am strongly in favor of adequate and as-liberty-respecting-as-possible eradication of covid.
The event space I care about for an infectious disease is the event space that represents the large scale long term summary statistic that cleanly models "the entire herd and its general health". It is a weird position, but... well... I'm honestly kind of surprised that even 2% of people agree with me? It isn't like I don't notice that I'm weird <3
Replies from: Daniel V↑ comment by Daniel V · 2021-12-09T16:01:53.928Z · LW(p) · GW(p)
Good job looking for cruxes! I agree with you that quantifying a differential in exposures would help nail down how much we should favor vaccination (or not), but the idea behind the probabilities I laid out was getting at the risk of inducing asymptomatic-spread. At the most unfavorable to vaccination (like how I also assumed vaccination leads to only asymptomatic disease), asymptomatics generate N infections from N exposures with p=1 and symptomatics generate exposures with p=0 (because they quarantine), so we can just look at the risk of inducing asymptomatic-spread without additional layers of calculation.
Though that does indeed depend on the key probabilities going into calculating the risk. If p>>5%, then additional calculation would be warranted, and calibrating the probabilities better would be more important. For example, it's clear just looking at the conditional probabilities that the turning point is when the relative risk of infection depending on vaccination equals the reciprocal of the relative risk of being asymptomatic conditional on infection depending on vaccination - that is, if vaccinateds are twice as likely to be asymptomatic conditional on infection than unvaccinateds (wow, the RR is a little under 2, but let's call it 2, Fig 3), we prefer vaccination as long as vaccination cuts the risk of infection by at least half (vaccine effectiveness >= 50%). Any less than half, and then we can't just prefer vaccination out of hand and have to go through and calculate. And then figuring out the actual differential in exposures (and viral loads!) would be relevant too.
I agree with you that the probabilities I'm focusing on are in a much narrower time frame and that widening it out, p will lift off from the rate estimated in the clinical trials (about a 2 month window). As the vaccine effectiveness rate approaches 0%, then indeed we can't prefer vaccination out of hand. How would that happen? As you suggest, with a long enough time window, the attack rates could equalize at 100%. I don't actually see that happening (I expect the vaccines don't only provide probabilistic protection of around 85% but, at least for some, effective immunity). But vaccine effectiveness could reach the reciprocal of the relative risk of being asymptomatic conditional on infection depending on vaccination well before getting to 0%. If you think vaccine effectiveness for the long term will fall below 50%, then we have some more calculating to do. Seeing as effectiveness has stayed about as high as models would tell you, falling below 50% only seems like a real possibility with Omicron, and my guess is we'll either get a new shot to avoid lower effectiveness [1] [2] or learn that 3 doses work against it.
My prior on vaccine effectiveness staying over 50% even in the long term is strong enough, and the extra research and calculation that would otherwise be required to address this further is daunting enough, that I'll leave it at that. I don't want to say the burden of proof is on either of us here, since ultimately it depends on which prior is "deemed" the prior.
I want to reiterate that your general point that a vaccine might not have the public good value we assume it has is legit. We are used to diseases that generate symptomatic infections with high p, so any reduction in symptomatic infection is noticeable and contributes to stopping the spread. If a vaccine pushes infections to "hide" in asymptomatic ones instead (because the disease generates symptomatic infections with low-moderate p), and asymptomatic infections are still highly transmissible, the public good value is not quite so certain, generally speaking.
↑ comment by cistrane · 2021-12-10T19:28:55.709Z · LW(p) · GW(p)
How do you incorporate unvaccinated who recovered from covid in your model? Are they equivalent to vaccinated?
Replies from: Daniel V↑ comment by Daniel V · 2021-12-11T01:48:15.918Z · LW(p) · GW(p)
They'd be vaccinated-lite. The neutralization titers in vaccinated plasma are better than in convalescent plasma. Lots of room to complicate things and get it closer to reality, but that doesn't touch the public good value thing so much.
Replies from: cistrane↑ comment by cistrane · 2021-12-11T06:09:29.930Z · LW(p) · GW(p)
You can do better than vaccinated lite. Since we know that neutralization titers in vaccinated decline as a function of time from vaccination, we can say that the unvaccinated recovered are like vaccinated ~4 months from vaccination, or 5 months and then we can treat everyone as vaccinated with x time passed from last vaccination.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-12-11T09:50:36.395Z · LW(p) · GW(p)
4 months since having the third booster provides more protection then 4 months since second shot.
A lot of vaccines out in the world are already 0, 1 months 6 months to give people good lifetime protection because two shoots are not enough to give lifetime protection.
Replies from: cistrane↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-06T23:14:43.150Z · LW(p) · GW(p)
Do you distinguish between "encouraging with an incentive" and simply encouraging? Similarly, where would "scolding or shaming" fit in?
And is it possible to disguise a mandate as an incentive? For instance, if we gave a million dollars to everyone who gets vaccinated and boosted, wouldn't that start to have a material impact on the CPI, forcing people to get vaccinated just to stay afloat?
Replies from: Pattern, cistrane↑ comment by Pattern · 2021-12-07T19:29:17.036Z · LW(p) · GW(p)
Where do I start.
1.
Example of "Encouraging": curfew for everyone not vaccinated (unless they have medical reasons to not).
Something as vague as 'encouraging' is rather unclear.
2.
And is it possible to disguise a mandate as an incentive? For instance, if we gave a million dollars to everyone who gets vaccinated and boosted, wouldn't that start to have a material impact on the CPI, forcing people to get vaccinated just to stay afloat?
A massive impact on the Consumer Price Index, in the outcome you outline.
It's possible. (The scenario you outlined seems unlikely - 1 million dollars?)
The point of your questions isn't entirely clear, which makes answering them difficult.
Yes, one could argue that an incentive that large is...kind of equivalent to a mandate in that few who are not at health risk would refuse, even many who would be at risk might take a gamble with their lives for that much. (Also, while many ideas around the vaccine being risky are ridiculous - microchips etc, such a surprising approach might prompt a re-evaluation. It also might hit supply, at least temporarily, as that could cause a large increase in demand.)
At the same time I haven't looked at CPI to see what it does and doesn't include. The economic effects would be large, though I'm not sure how exactly things would change.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-08T09:47:06.867Z · LW(p) · GW(p)
Aw, thanks for answering despite the point not being clear! Guilty as charged! Respect for answering them anyway!
"We choose to go to the Moon in this decade and do the other things, not because they are easy, but because they are hard" - JFK
comment by Annapurna (jorge-velez) · 2021-12-06T20:03:03.418Z · LW(p) · GW(p)
New Omicron market on Polymarket:
https://polymarket.com/market/will-at-least-10pct-of-us-covid-19-cases-be-from-the-omicron-variant-on-january-1-2022
comment by NoSignalNoNoise (AspiringRationalist) · 2021-12-07T01:48:34.668Z · LW(p) · GW(p)
Either it’s bad or weird data, or Omicron somehow puts a ton more virus into the wastewater, and then there’s nothing to see here.
If Omicron somehow puts a ton more virus into the wastewater, that tells us something interesting about the virus. Maybe it somehow infects the digestive tract more effectively than other strains.
Replies from: TheSimplestExplanation↑ comment by TheSimplestExplanation · 2021-12-10T17:34:37.296Z · LW(p) · GW(p)
Or it has a higher viral load.
comment by ESRogs · 2021-12-07T23:38:55.791Z · LW(p) · GW(p)
Any thoughts on the speculation that Omicron may be the result of a new lab leak from a lab in SA experimenting on immune escape?
(I have not read the paper cited in that tweet in depth, and I don't know anything about the tweet author. But superficially, their thesis sounded plausible.)
↑ comment by TheMajor · 2021-12-08T00:14:03.336Z · LW(p) · GW(p)
The paper seems to describe the Delta variant and classify its properties compared to older strains. I'm not an expert so I might well be misunderstanding it, but that paper seems to classify and compare two wild strains, not modify them? Maybe I'm missing something, but what is the relation with omicron?
I thought the fact that South Africa does far more sequencing than other countries in that part of the world (for example, check the reported Delta sequences by country, where South Africa is listed as 25th globally with 11,004 sequenced samples, and the next sub-Saharan country seems to be Nigeria, 49th, 2,075 sequenced Delta samples) is more than sufficient to explain away the surprise that they noticed it first. The fact that they also have a laboratory for virus research is hardly a coincidence.
As far as I know there is insufficient evidence to assume omicron is lab-created, as opposed to, for example, reverse zoonosis or long development time inside a person with a compromised immune response. But even conditional on omicron being lab-created, what reason is there to assume it originates from a lab in South Africa? The twitter threat does not seem to provide an answer.
Replies from: ESRogs↑ comment by ESRogs · 2021-12-08T00:53:29.291Z · LW(p) · GW(p)
I'm not an expert so I might well be misunderstanding it, but that paper seems to classify and compare two wild strains, not modify them? Maybe I'm missing something, but what is the relation with omicron?
I think the conjecture is that the virus would have mutated on its own, in the presence of antibodies. But on second thought, maybe that's relatively unrealistic (as a possible explanation for Omicron), because we'd expect much more mutation in the wild where there are much higher quantities of the virus?
comment by Sammy Martin (SDM) · 2021-12-07T16:02:32.340Z · LW(p) · GW(p)
If you have good news sources and follows to keep a better eye on the UK or Europe for Covid purposes, or data sources anywhere I may not have noticed, I invite you to share them in the comments.
James Ward is good for factual UK based covid news and especially as an aggregator of other news sources. His new thread on prospects for the Omicron variant is here.
comment by wunan · 2021-12-06T23:18:25.611Z · LW(p) · GW(p)
What do you mean by "immune erosion"? Is this different than "immune evasion" and "immune escape"? I can't find any explanation on google -- is this a standard term?
Replies from: caridorc-tergilti, cistrane, bww↑ comment by Caridorc Tergilti (caridorc-tergilti) · 2021-12-07T09:35:41.009Z · LW(p) · GW(p)
Immune erosion is used to make people understand that immune escape is only partial and not total
↑ comment by cistrane · 2021-12-10T19:36:35.805Z · LW(p) · GW(p)
Existing mRNA vaccines theoretically provide antibodies to about 42 epitopes of the original spike protein. So, they are very effective against the original strain as any one of these antibodies would be neutralizing.
Let's say for example that only 10 out of 42 are neutralizing for omicron. That means that many people will be unlucky and not produce enough of the right antibodies to stop the omicron at first, thus their protection has eroded. But some will be lucky enough to produce the necessary amount of the right antibodies. So the protection was not completely bypassed.
↑ comment by bww · 2021-12-07T04:08:51.775Z · LW(p) · GW(p)
Per my understanding "immune evasion" and "immune escape" imply a binary, i.e. previous immunity has no effect. "Immune erosion" is a more intuitive way of describing how this variant likely interacts with protection from previous infection or vaccination, with protection against infection, hospitalization, death "eroding" to a degree but not being completely negated.
I believe I first saw it in this twitter thread: https://twitter.com/kakape/status/1428657737190322184?s=20
comment by MondSemmel · 2021-12-06T19:06:06.842Z · LW(p) · GW(p)
If that’s the attitude of the CEO of Pfizer, that should both put to bed any rumors that the vaccine companies are trying to trick us into taking extra vaccines to make them more money
Correction: It's the BioNTech CEO.
Replies from: Zvicomment by Liam Donovan (liam-donovan-1) · 2021-12-07T02:34:06.637Z · LW(p) · GW(p)
Wait, how do you get to 17%-25% chance of a crisis situation if there's only a 2.5% chance of omicron causing severe disease in vaccinated/previously infected people? Isn't that the vast majority of people in the US?
Replies from: Bucky, gabriel-holmes, arunto↑ comment by Bucky · 2021-12-07T11:41:47.175Z · LW(p) · GW(p)
My understanding is that a few months after vaccination the vaccines provide ~85% (?) protection against hospitalisation compared to an unvaccinated person.
I think the 2.5% prediction is intended to indicate that Zvi thinks it's highly unlikely that this will drop to 20% protection from Omicron (or similarly low number). However even a drop to 70% (which seems more reasonable) would mean a doubling of hospitalisations per case.
Even with this, my model of a crisis situation is more to do with a huge increase in infections than with increasing hospitalisation rates per case.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-09T08:22:39.598Z · LW(p) · GW(p)
Because there aren't enough hospital beds/nurses etc
↑ comment by arunto · 2021-12-07T09:17:27.513Z · LW(p) · GW(p)
Isn't that the vast majority of people in the US?
We know the vaccination rates (NPR). And we have estimates for the the number of infected persons (Estimated COVID-19 Burden). But do we have a trustworthy estimate for the intersection of those two groups (and with that an estimate for the total number of previously infected and/or vaccinated)? That would be important information, ideally statewise.
The other important data point would be the intensive care capacity.
Replies from: cistrane↑ comment by cistrane · 2021-12-10T19:41:40.323Z · LW(p) · GW(p)
We could start by naively assuming that recovering from covid infection and vaccination against covid are completely independent. For a state with 50% vaccination rate, there would be 50% of the unvaccinated and about half of all unvaccinated would be previously infected.
comment by Phil · 2021-12-06T23:54:32.363Z · LW(p) · GW(p)
One thing I've never found the answer to: is a positive test evidence of disease? It seems to me that a vaccinated person inhales the virus just as readily as an unvaccinated person, but the vaccinated person's immune system fights it off before symptoms (or before serious symptoms) appear.
In that case, wouldn't it be normal and expected for vaccinated people to sometimes test positive, in the sense of "there exist copies of the coronavirus in the upper respiratory system"?
↑ comment by Elizabeth (pktechgirl) · 2021-12-07T00:10:46.285Z · LW(p) · GW(p)
People become more contagious as there are more viral particles in their system. Vaccination inhibits replication (but less than 100%), so you would expect a vaccinated person to have a lower viral load after exposure than an unvaccinated person. They might also have more symptoms, because some symptoms are immune responses and the whole point of vaccination is to give you a stronger response at an earlier viral load.
Replies from: ChristianKl, gabriel-holmes, Phil↑ comment by ChristianKl · 2021-12-07T12:49:45.418Z · LW(p) · GW(p)
Vaccination inhibits replication (but less than 100%),
But not automatically everywhere in the body. To inhibit replication in the upper respiratory system you need mucosal immunity.
RaDVaC could potentially provide that but the approved vaccines don't. The approved vaccines only give you a response once the virus attacks deeper parts then your upper respiratory system.
↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-07T10:36:27.804Z · LW(p) · GW(p)
I may have experienced this last week, after having a mild sub-detectable exposure. It felt a lot like after shots 2, 3 and 4. But I still haven't tested positive.
↑ comment by Phil · 2021-12-07T00:18:02.374Z · LW(p) · GW(p)
Is the vaccinated person's lower viral load enough to trigger a positive test, especially for those with symptoms?
If it is, shouldn't we be thinking of "reinfections" as those cases of serious disease, rather than simply positive tests?
↑ comment by Elizabeth (pktechgirl) · 2021-12-07T02:17:41.421Z · LW(p) · GW(p)
There is no one vaccinated person. Getting a load high enough to trigger a positive test is less likely but still possible post-vaccination. The interaction with symptoms is weird because symptoms are caused by both viral load and immune response.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-09T08:19:51.827Z · LW(p) · GW(p)
This lends credence to my theory about last week's exposure. Six negative rapid antigen tests and two negative PCR tests over the course of the seven days following the possible exposure, but I felt like hell about three days after.
↑ comment by tslarm · 2021-12-07T00:17:49.913Z · LW(p) · GW(p)
(disclaimer: no expertise)
I don't think any of the tests are expected to return a positive result when the tested person's viral load is extremely low. You can get a positive result and remain asymptomatic, but I think that's only supposed to happen when the virus has got into you in a meaningful way, i.e. multiplied itself a bunch of times -- not when you just happen to have recently breathed in a few virus particles.
as a quick citation, see the data here on false negative rates: https://www.nature.com/articles/s41598-021-88498-9
Replies from: Phil↑ comment by Phil · 2021-12-07T00:21:35.154Z · LW(p) · GW(p)
Fair enough. The question is then, does a vaccinated person's immune system take care of the virus so fast that the viral load remains "extremely low" enough to result in a negative test?
That seems counterintuitive given that Elizabeth says vaccinated people are more likely to be symptomatic, but I suppose it's possible that the immune system would trigger covid-19 symptoms even while maintaining a low viral load.
↑ comment by tslarm · 2021-12-07T00:31:17.531Z · LW(p) · GW(p)
My model is that the vaccine basically gives your immune system a head start, so your chances of each of the following (conditional on a better outcome not having already happened) are higher than they otherwise would be:
- clearing the virus before it replicates enough to be noticable, either via symptoms or a positive test;
- clearing the virus after it is noticeable, but before anything serious happens;
- clearing the virus after it causes serious disease, but before it kills you.
So the answer to your question would be 'sometimes' -- more often than if they were not vaccinated, but of course non-vaccinated people do it significantly >0% and vaccinated people significantly <100% of the time.
(Sorry if this misses your main point, btw -- I'm not being deliberately obtuse, I'm just not completely sure what your broader point is, so I'm focussing on the specific questions.)
comment by frankybegs · 2021-12-08T23:13:20.282Z · LW(p) · GW(p)
How can you say it's a coin flip, but also "the people saying there's no evidence [of the affirmative] have no leg to stand on"?
Sure, literally speaking, there is some evidence.
But as far as I can tell, when people say 'there's no evidence that x' they don't mean that there is literally no evidence. There is some shred of compatible evidence with almost everything- with all sorts of ridiculous things that no-one rational believes.
As far as I can tell, when someone says there is 'no evidence for x' they mean that there is no evidential basis to believe x. The evidence doesn't give you any reason to prefer the hypothesis.
That seems to me like a vaguer, and probably less useful, way of taking essentially the same position as yours. It kind of proves the benefit of putting concrete probabilities on things, but I don't think it's all that substantively different from your position.
comment by frankybegs · 2021-12-08T19:41:39.911Z · LW(p) · GW(p)
Note how crazy it is that there are 68% of people support mandatory vaccination but only 70% (2% more!) people support encouraging booster shots. There are almost no people with the ‘encourage people to do useful things but don’t force them to do those things’ position. Sigh.
This seems almost wilfully cynical, given that the poll actually says 'COVID vaccination requirements'. That's quite vague, and could plausibly not be all that much different from 'encouraging booster shots', e.g. if full vaccination is a requirement to enter certain events and venues.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-12-09T20:14:32.652Z · LW(p) · GW(p)
I wonder if there's a subset of the population for whom Evusheld might eventually either
- Count as vaccination
- Be mandatory in order to be considered immune
comment by tkpwaeub (gabriel-holmes) · 2021-12-07T10:29:11.031Z · LW(p) · GW(p)
Some insight into the transmissibility - Omicron made its way from one hotel room to another. The occupants had no contact.
It still doesn't quite answer the question of what the exact physical characteristics are that allow it to be this transmissible (smaller? Stickier? More likely to linger in the air or fill up a space uniformly?)
Which makes me suggest another "side bet" - what's the probability that Omicron is so transmissible that any attempt to contain it is an exercise in futility?
comment by Oskar Mathiasen (oskar-mathiasen) · 2021-12-07T10:38:22.649Z · LW(p) · GW(p)
Repost from my wordpress comments:
Danish seroprevalance (from https://www.ssi.dk/aktuelt/nyheder/2021/markant-stigning-i-den-fjerde-nationale-praevalensundersoegelse) seems to have been about 50% above commulative cases (from https://www.worldometers.info/coronavirus/country/denmark/) by may 2020.
Commulative omicron cases in Denmark per SSI https://www.ssi.dk/aktuelt/nyheder/2021
dec 3: 18 omicron cases
dec 5: 183 cases
dec 6: 261 cases
Oddly this looks linear (80 cases per day), but that is almost certainly random.
↑ comment by Oskar Mathiasen (oskar-mathiasen) · 2021-12-07T15:18:22.719Z · LW(p) · GW(p)
Todays cumulative omicron cases is 398
Replies from: cistranecomment by Annapurna (jorge-velez) · 2021-12-06T18:40:06.077Z · LW(p) · GW(p)
Hey Zvi, do you accept tips through Polymarket?
Replies from: Zvi↑ comment by Zvi · 2021-12-06T19:14:20.028Z · LW(p) · GW(p)
I did not know such a feature existed, say more?
You can subscribe to the substack (thezvi.substack.com) or use my Patreon (https://www.patreon.com/thezvi) if you'd like to contribute.
Also considering turning on Twitter tips, which I think would have relatively low fees.
Replies from: ipike, Zvi, jorge-velez↑ comment by nomiddlename (ipike) · 2021-12-07T13:34:18.936Z · LW(p) · GW(p)
I think the ‘Polymarket address’ is really your ethereum address. People can use that to send tips over the matic network (the network polymarket is on which uses ethereum addresses) for probably less than a cent in fees.
↑ comment by Annapurna (jorge-velez) · 2021-12-06T20:02:27.442Z · LW(p) · GW(p)
If you use the platform, just link your polymarket address and people can peer to peer you tips at no cost.