Omicron Variant Post #1: We’re F***ed, It’s Never Over
post by Zvi · 2021-11-26T19:00:00.988Z · LW · GW · 95 commentsContents
The First Three Times If Omicron Is What We Think, We Cannot Stop It, Only Slow It Down Travel Restrictions Lockdowns Vaccinations Biological Priors What Do We Know About Omicron? What’s Going on in South Africa World Reaction Current Model Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 30%. Chance that Omicron will displace Delta: 70%. Chance that Omicron is importantly more virulent than Delta: 25%. Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 50%. Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 5%. Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 15%. Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 5%. Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 20%. Final Thoughts None 95 comments
The last day has seen the imposition of new travel restrictions and spreading alarm about the Omicron variant. It sure looks like a repeat of what happened with Alpha and Delta, as well as the original strain back in early 2020, and that we are probably doing this again.
How will this play out this time? It’s very early. There’s tons of unknowns. Yet there is a lot we can say already, and many actions need to happen now to have any hope of doing much good. So it’s time to move fast, see what we can say right now and try to capture the speed premium.
I’ll start with a summary of what we know about the game board based on previous experience, then look at what we know about Omicron and what moves have been played so far in this round.
I was almost finished with this post when the WHO decided to go with Omicron instead of Nu (or even Xi) and then I had to go through and replace Nu with Omicron about 25 times. We could have just said ‘the Nu variant’ a lot but the WHO hates both efficiency and fun even more than it hates freedom, it seems. Sad.
The First Three Times
In early 2020, we got warnings about a new potential pandemic. Almost all reactions were too little too late. What warnings I offered were less too late than most, but still too tentative and too late.
About a year ago, as the Alpha variant was spreading, it seemed like the same pattern was happening again. It was clear Alpha would take over. I extrapolated into the future, did the math as best I could, wrote the post We’re F***ed, It’s Over, noted the unknowns, and predicted a 70% chance of a large wave between March and May.
As I noted in the later update, it was not over. There was no big wave between March and May of 2021. Alpha wasn’t as additionally infectious as I expected, but it wasn’t that much less additionally infectious than I expected, and I didn’t have enough respect for several factors including seasonality. In hindsight the 70% prediction was somewhat overconfident, and a prediction of about 45% would have been better.
Then, as it looked like things would have otherwise died down and normal life resumed, Delta arrived. It was quickly clear it would not be contained for long and Delta would take over. The situation in India seemed super scary, with hospitals overwhelmed and the serious possibility Delta would sweep through the entire population, first in India and then around much of the world.
Then India’s situation stabilized quickly, and it seemed clear we had sufficient vaccinations plus control system reactions to prevent things from getting too far out of hand. There would be a wave now, perhaps another in winter, but it would not be a crisis.
Winter is now coming, and that winter wave is clearly already underway, except now we are likely to also face the Omicron variant.
If Omicron Is What We Think, We Cannot Stop It, Only Slow It Down
Before we get to the details of the Omicron variant, it’s worth taking a step back and asking what we know about such developments in general, and how things are likely to play out and what options might be available.
The first point is the obvious one. There is no stopping a variant that is substantially more infectious than Delta. If Omicron is indeed substantially more infectious than Delta, it will become the dominant strain throughout the world.
Once there are hundreds of detected cases, it is already far too late to successfully contain the new variant. By the time we have enough information to react to a new variant, there will already be hundreds of detected cases. We lose. Good day, sir.
That doesn’t mean there are no physically possible measures that could contain the new variant once there are hundreds of detected cases. It does mean none of them are remotely in the Overton Window, or logistically within the abilities of our governments even if they decided to try anyway. Playing to win the game is not an option here. We lose.
That doesn’t mean we can’t or shouldn’t do things that make us lose slower. We can absolutely slow down the pace at which Omicron displaces Delta.
Whether or not that time is useful depends on what we do with that time.
Perhaps not very much time. The worse Omicron is, the more rapidly it will take over and the less time we can buy with countermeasures. In practice, in terms of the takeover rather than the overall number of infections, we could likely buy ourselves a week or two, but it’s hard to see us buying more than that. We could also institute general restrictions against Covid-19 to reduce the number of infections across the board. Once again, we buy ourselves a small amount of time.
If buying time before a sufficiently large wave gets us better access to Paxlovid or other treatments, or allows us to get a lot more people booster shots that still work, or time to make a new version of the vaccine and roll it out, time can be quite valuable.
There’s also the possibility of stalling to get better seasonality effects when crunch time happens. The wave maxing out in December seems like maximally bad timing, and we’d prefer to push it to January or February.
If you buy time and then it is wasted, then nothing is gained. If you pay a big price to buy time, it needs to be paired with a similarly big effort to make use of that time.
Travel Restrictions
The first step is always a debate over travel restrictions. Travel restrictions feel like Doing Something, and failure to impose such restrictions opens the door for blame.
When the WHO warned against travel restrictions, that’s when I knew in my gut what we were dealing with.
Travel restrictions are an excellent idea when the goal is to buy time. They can definitely slow down the rate at which the new variant spreads across borders.
What they can’t do is stop it entirely, even if they are imposed early enough, unless you’re sufficiently serious.
Sufficiently serious means actually closing off or at least aggressively quarantining everyone who has any exposure to the areas in question, which includes any areas not taking similar measures, anywhere. There can’t be exceptions, including for your citizens.
Realistically, your minimum case that could possibly fully work is to be Australia, and quarantine everyone at the border even if there’s no reason to suspect anything, and you need to do it right. That’s not going to happen.
Even if you did succeed, what then? How long are you going to keep your borders closed? A restriction to a few countries might help the first week, but within a month it won’t even much matter, because there’s too much spread elsewhere. It’s not like a variant worse than Delta is going to go away any time soon, so you’re stuck in a permanent state that in most places both can’t be created and can’t be sustained if you did create it.
For those places that showed they can sustain it, would you even want to, and for how long? When would it end? What’s your plan?
The other issue with travel restrictions is they continue long, long past the time when they still make any sense. Once containment has generally been lost, the restrictions don’t do anything. At a minimum, they do nothing unless you’re in a much much better place than the region you’re cutting off, whereas there were many cases of longstanding mutual restrictions where the same variant was dominant in both places, which is pure folly.
It does seem like ‘impose travel restrictions aggressively to buy time’ is a good response. The short term cost is very low, and with so many unknowns the upsides are very high. If you do that, you need to do it very quickly. The best time is a week ago, the second best time is right now, and all that. In the scenarios where it matters most, a week from now there won’t be much point.
Exactly what restrictions are imposed by who, and when, provides strong insight into how various governments respond to new information.
Lockdowns
It’s worth noting that if a new variant is about to displace the old one, then lockdowns designed to stop the spread of the old variant are much less worthwhile. Once there’s a displacement event, the previous infection level no longer matters at all. If anything, previous infections could be an advantage, if the new variant is more dangerous, and/or it means the spread can be slowed down due to natural immunity. The flip side is if somehow natural immunity was going to stop working entirely against the new variant, then every case prevented in the meantime is a pure extra case, which based on history seems unlikely but is possible.
The bigger reason to reconsider existing lockdowns is that there are increasing marginal costs for lockdowns, and a limited capacity to impose them. The early efforts to stop the spread ‘used up’ a lot of that capacity. Lockdowns now, before the crunch time, could end up having little effect and also making it impossible or more expensive to lockdown again later when it matters most. To the extent that lockdowns are a good idea, they need to be timed carefully.
The counterargument to that is that a lockdown suppresses overall transmission levels of the new variant as well. Even if you have only 10 cases, if you slow down spread from those 10, that’s worth a lot and buys you time. That’s true, but mostly only works if you’re no longer importing meaningful numbers of cases from elsewhere, and for various dynamic reasons the amount of time you buy here won’t be very large.
You can also attempt to do a lot of sequencing, then do aggressive quarantines and contact tracing when you find the new variant, but the capacity to do this enough to matter is not present.
Vaccinations
The best defense against prior waves and variants has been vaccination. Every time a new variant arrives, fears are stroked that the vaccines will stop working, or will be less effective.
Despite that, we’ve had months in which we could easily have updated the mRNA vaccines to fully match the Delta variant, we are now giving out booster shots even, and still no sign of any attempt to modify the vaccines.
I’m unsure how much evidence this is against the need to update the vaccines. If the vaccines had stopped working entirely, or taken a sufficiently strong hit, presumably we would have updated to a new version. The FDA has promised to look kindly upon such changes, and it seems like it could only help on both health and financial considerations. My guess is it’s actually quite a bit of evidence against any strong potential gains from updating, but weak evidence against weak gains.
So far, all talk of immune escape has mostly been exactly that, talk. That should make us wary of expecting it out of a new variant, or of updating too much from people’s concerns.
If a new variant comes along that does offer substantial escape from the vaccines, we will need to update the vaccines and get new versions out as quickly as possible. Will we be able to do that?
Technologically I have no worries. We’ll have that part solved within the week and probably within one day.
Engineering I’m also not worried about. My understanding is this is at most a two week process. There are still concerns about rate of production, since we were stupid enough not to scale this up enough in advance, but we’ll take whatever we can get.
It therefore comes down to the FDA making good on its word to allow this to happen, and then on our ability to distribute the new boosters and communicate effectively why they are necessary and get people to accept them. In the short term, we don’t need to worry that much about communication, so that has more time to get its act together.
The other worry is that if Omicron is sufficiently worse than Delta, especially if it combines being otherwise worse with immune escape, the amount of time available might be quite short. Even if everything went smoothly the full process would still take months. We could go faster in theory, but that would require efforts on a different level than we made the first time or have accomplished in a long while on anything. I’m not optimistic.
Biological Priors
When we see a new variant spreading rapidly, what should our priors be about its biological properties?
Note that these are all things we should think are likely rather than anything that we know.
We have explored various potential mutations a lot by now, so we should put a lot of weight on what those mutations imply about the variant’s likely behavior.
We should presume that if something takes over quickly, it has a very large advantage infecting people who are unvaccinated and lack natural immunity.
We should presume that if it also has an additional property of vaccine escape, that seems like quite a coincidence, so it seems unlikely.
We should consider this even more unlikely if the variant started out in places with low vaccination rates.
We should also presume immune escape from either natural infection or vaccination is unlikely from our track record of Alpha and Delta not having this property.
We should presume there will still be more ‘breakthrough’ infections but that this comes from the protection levels no longer being sufficient because the new variant is easier to catch in general, not because the particular protections you have stopped working.
We should presume at this point some positive correlation between infectiousness and virulence, since both are likely tied to how much virus is typical (viral load), and previous variants followed this correlation.
We should be more confident in these things if our tests still work than if they start to fail.
What Do We Know About Omicron?
There have been a bunch of threads attempting to answer this question.
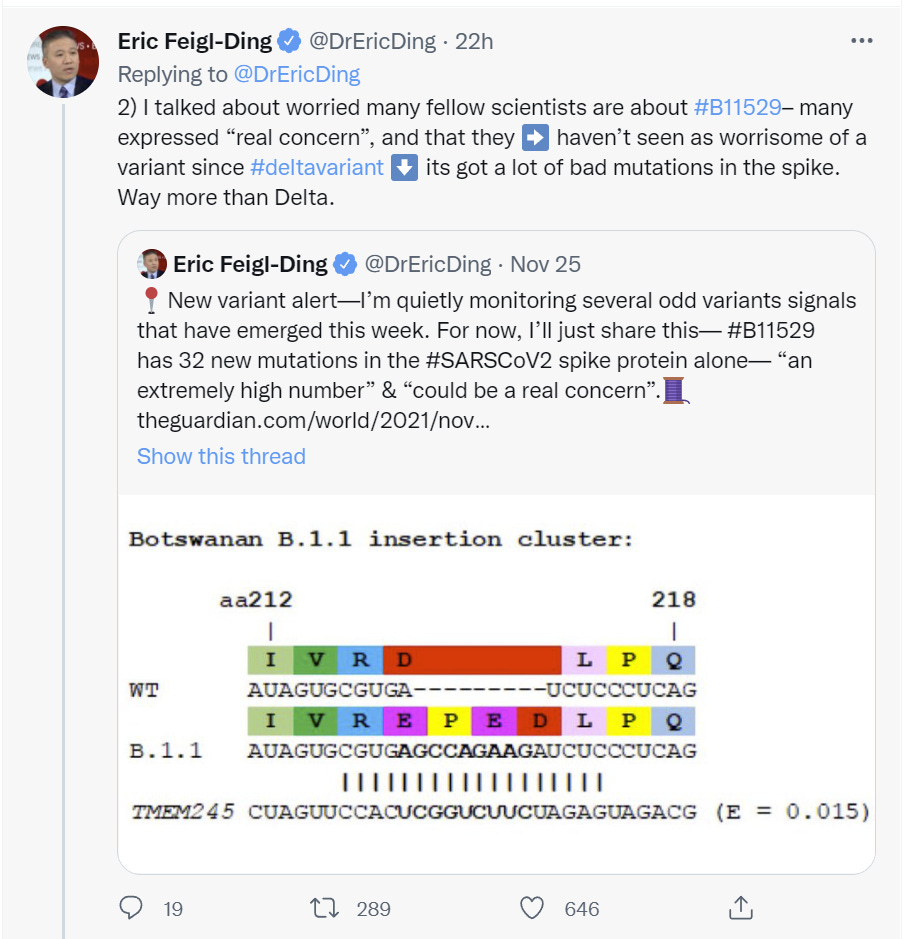
Here’s Eric Feigl-Ding, from Thursday around noon (things are moving rapidly, so timestamps are important).
I’m going to err on the side of directly putting in too much of these threads rather than too little, in the interest of speed, and to offer an easy option to get closer to the sources.
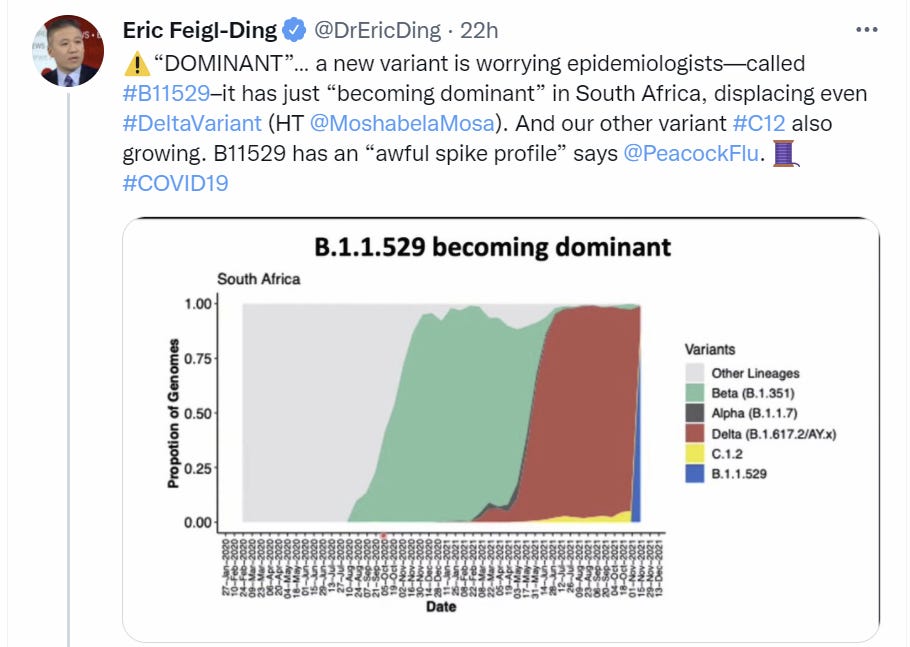






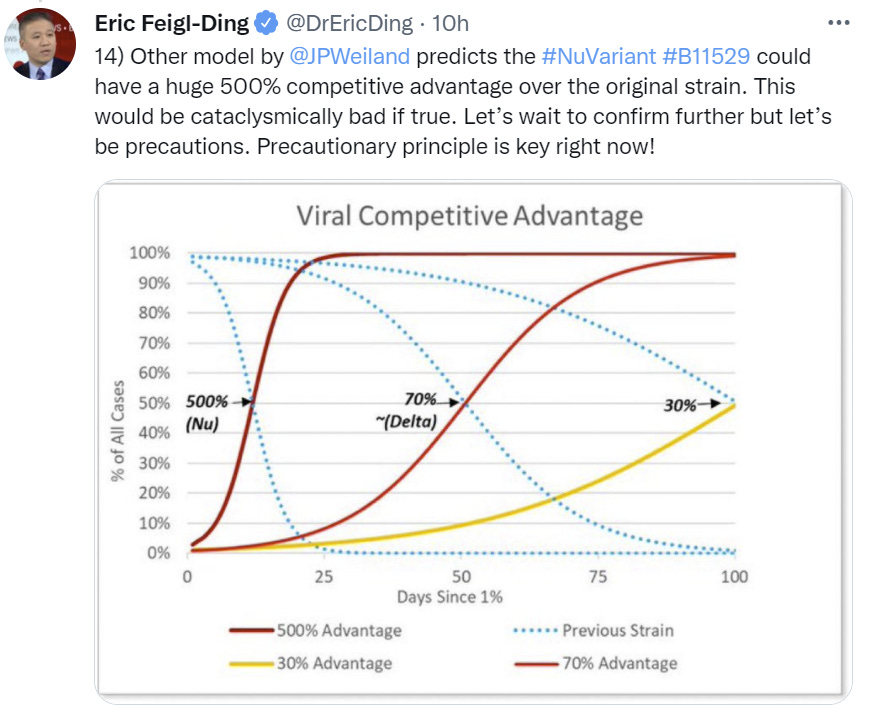
I think this final graph is a bit confused here, unless ‘the original strain’ here means Delta. Delta had about a 120% advantage over ‘the original strain’ or 70% over Alpha. I’m going to take this to mean 500% as compared to that 120%, so 600% of original versus 220% of original, or about a 170% additional increase. Which is… better, but still quite a lot.
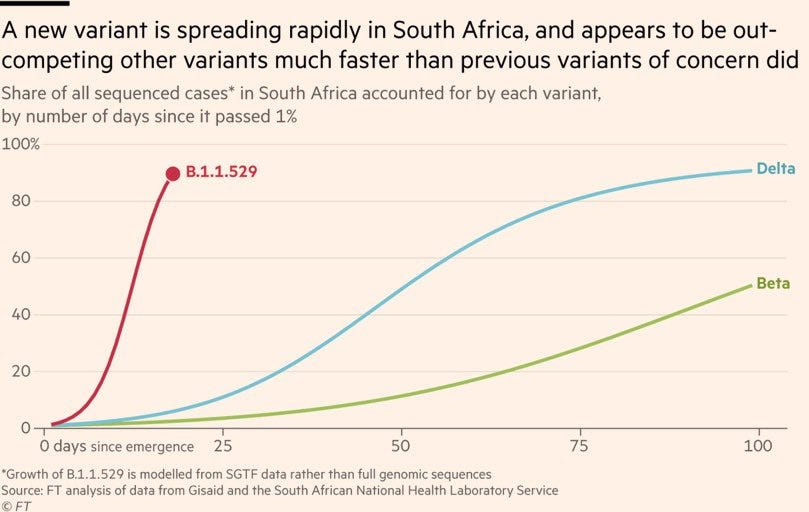
The graph above it does seem to imply that the Omicron advantage over Delta is being modeled here to be several times larger than the Delta advantage over Alpha/Beta, where ‘modeled here’ means looking at share of all cases in the country over time. This is a super scary graph, assuming it is accurate.
There’s also always the question of how this interacts with immune escape. Again, I’m using a baseline assumption that this is the same factor across the board regardless of level of immunity, and there isn’t an additional effect from escape of some kind.
South Africa’s vaccination rate is sufficiently low, and this rate of spread so high, that it wouldn’t much matter if there was vaccine escape properties, although it would presumably matter if there was escape from natural immunity.
Straight talk: If it’s 500% above Delta, in the way I understand it, We’re F***ed and it really really is over. At that point, it’s pure mitigation, and trying to flatten the curve a little bit, but yes everyone who isn’t immune is going to get this, and it would happen quickly. Under conditions where Delta would have had stable case counts, assuming a four day serial interval, this runs its course in America starting from a single case in about 50 days. If we assume 5 days per cycle, we get two months. Probably get somewhat more than that due to geographical barriers. There’d be a lot of attempted heroic prevention in the second half of that (the overall case number impact gets noticeable around the halfway point) and in particular in the endgame but in practice I doubt it much matters.
If it’s 170% above Delta, it changes how much time we have, and opens the door to meaningful action being possible to make things less awful. In particular, it gives a real shot to Paxlovid to be able to scale up in time to matter.
As always, such numbers are placeholders, approximations that simplify and mislead. Things aren’t that simple.
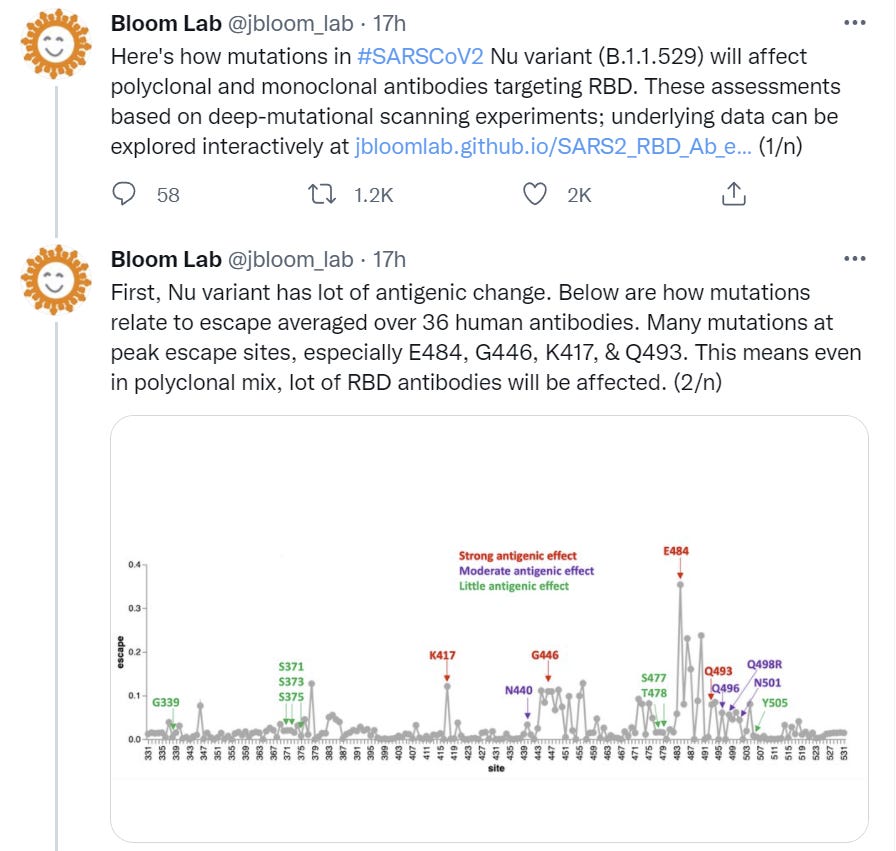
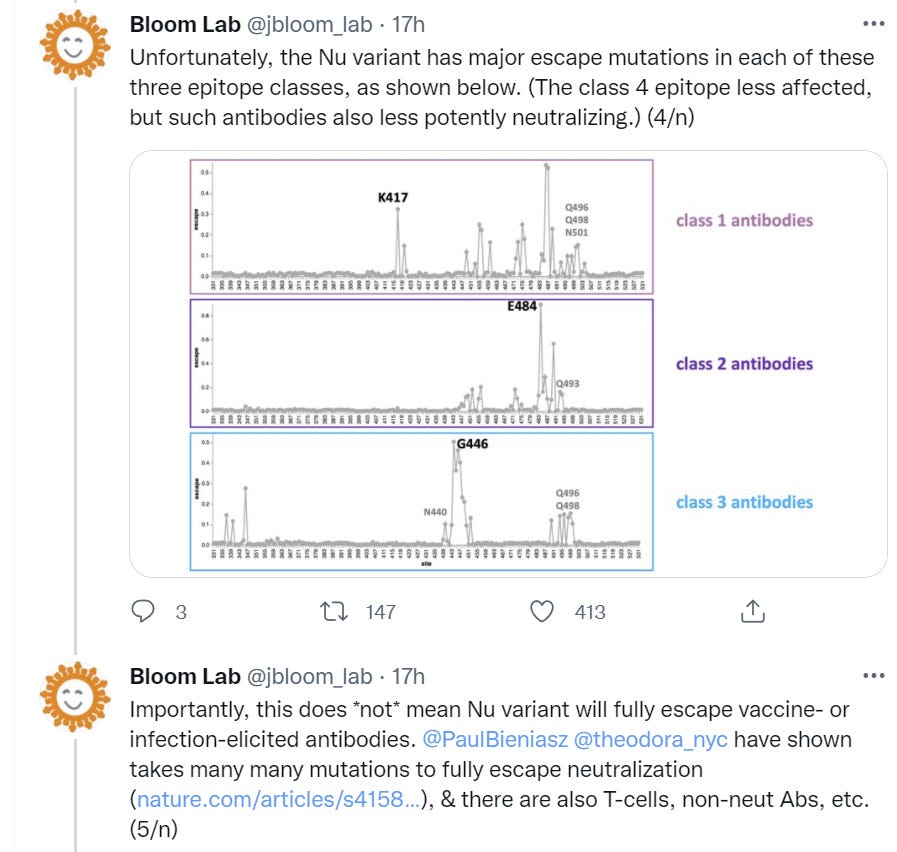
Here’s Bloom Lab, on the physical details:





This is the Trevor Bradford thread. He concludes that selection from vaccinations did not drive variants in 2021, but that conditions are changing and such selection grows more likely over time.
This is an argument that the advantage that Omicron has comes largely from its escape properties – it has tons of escape properties, and South Africans can have lots of natural immunity even if they don’t have a high vaccination rate, which is leading to the rapid spread.
Note that while I don’t put zero stock in differential impact on natural immunity versus immunity from vaccination, I don’t put much probability mass there either. I’d presume until proven otherwise that they both will weaken about as much as the other.
I’d also presume that since vaccination without boosters is mostly sufficient to protect against severe disease, and boosters provide a gigantic boost to protection on top of that, and this is not going to fully escape, that a booster should still be sufficient to offer practical protection against the variant, and non-boosted vaccination should still provide strong protection although potentially not as robust as before.
Note that this being about escape is in some ways good news. If it’s about escape, then we don’t have any reason to presume that the new variant is deadlier, or presents something we can’t defend against by renewing our defenses.
I also don’t see any reason to think that any of this would make Paxlovid or other non-antibody treatments less effective, so we’ll still have all of that in our arsenal.
Then again, Bloom Lab points out that there’s a contrasting viewpoint, and some chance it’s worse than all that, although I’d still consider it highly unlikely:

This thread calls for help for South Africa to ‘help contain’ the virus, and to avoid ‘isolating’ the country. I don’t see how one could hope to contain anything at this point, regardless of help, or how not isolating could make sense. The call to provide other kinds of help seems right.
Here’s the final big thread that seemed worthwhile.
Link above is to the 7th post in the Bloom thread above, below to the 2nd one.

This seems like the reasonable skeptical take. Things could be quite bad on any number of fronts, but we don’t know much yet. I agree that any pronouncements on severity should be treated with even more extreme skepticism.
Putting it all together, it seems likely that at least some of the advantage here comes from escape, or what Kai prefers to call immune erosion, but that we can be confident that this will only be partial.
We can’t be sure how much additional transmission advantage Omicron will have on top of that, but the Hong Kong case is suggestive given there are so few other cases abroad, and this level of rapid spread seems unlikely to happen only (or even primarily) from immune erosion properties. In the scenarios where the growth rate is ‘real’ in the sense that it reflects a very high transmissibility advantage for Omicron, I’d be very surprised if it wasn’t better at spreading among the unvaccinated never-infected.
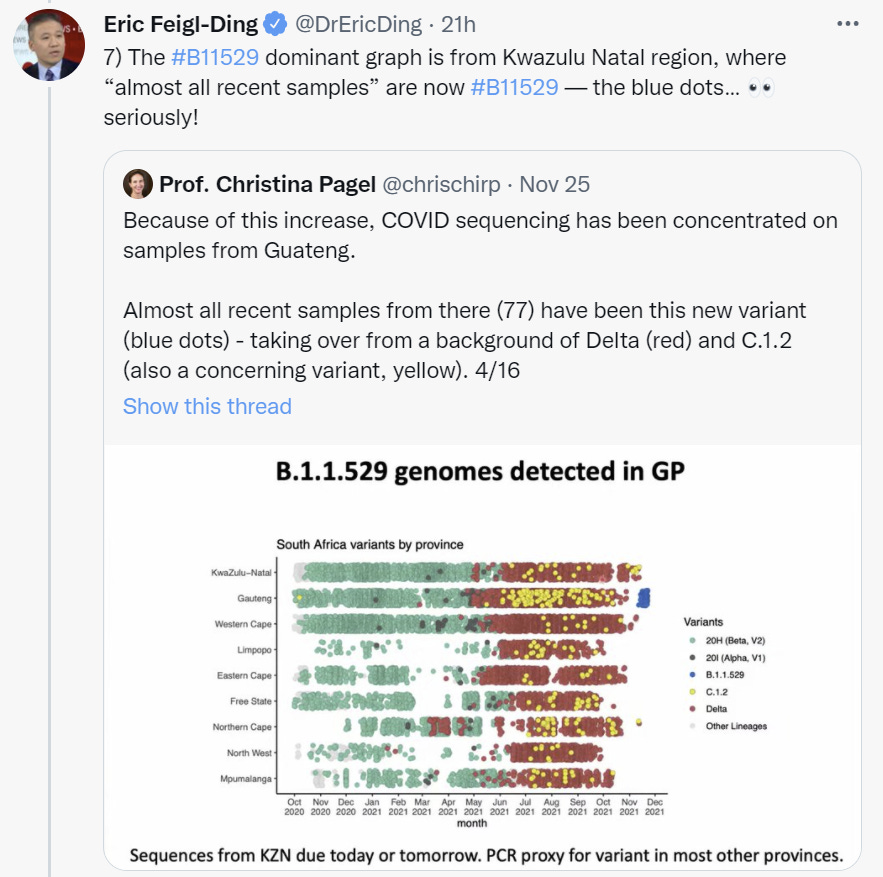
What’s Going on in South Africa
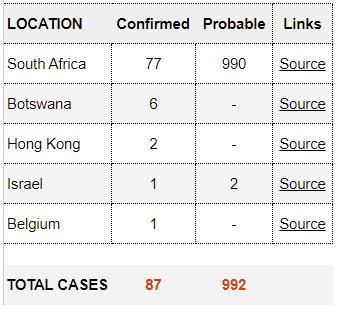
Concretely here’s the situation:

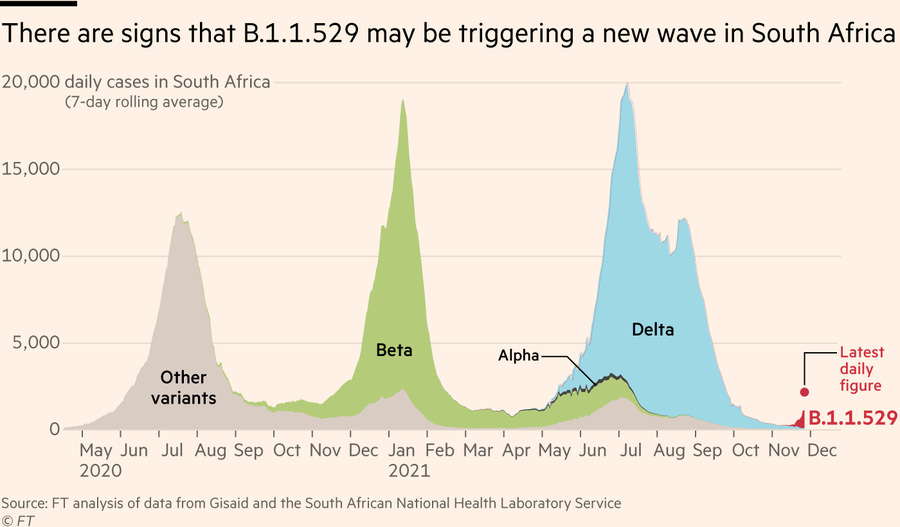
That’s not a very large red area on the right, but it is a very rapid rise. Still a chance this is all a blip. We will know more very soon.
The overall levels are still small, compared to places like the United States:
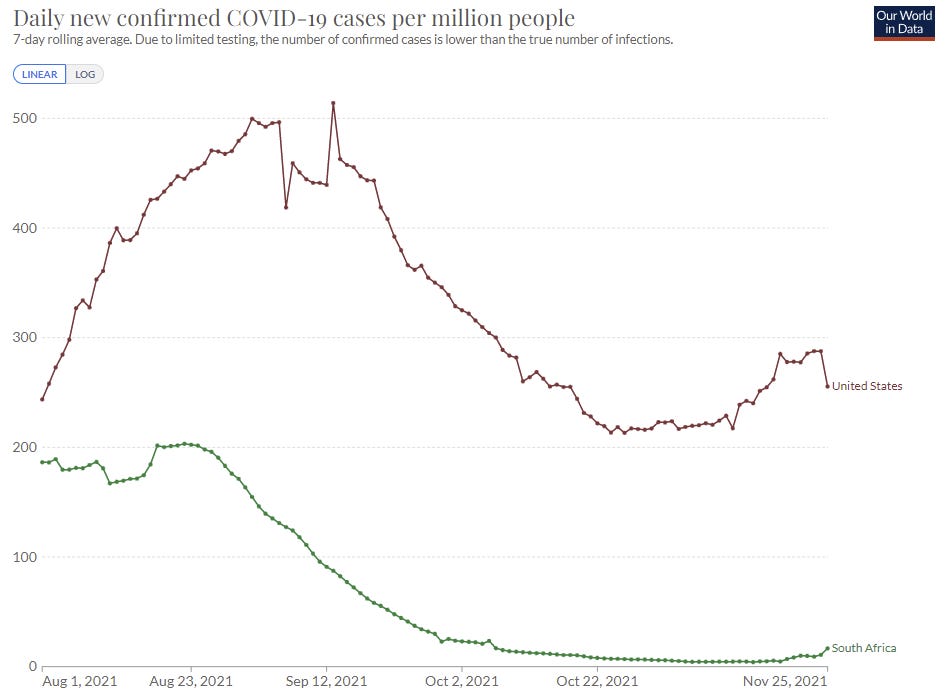
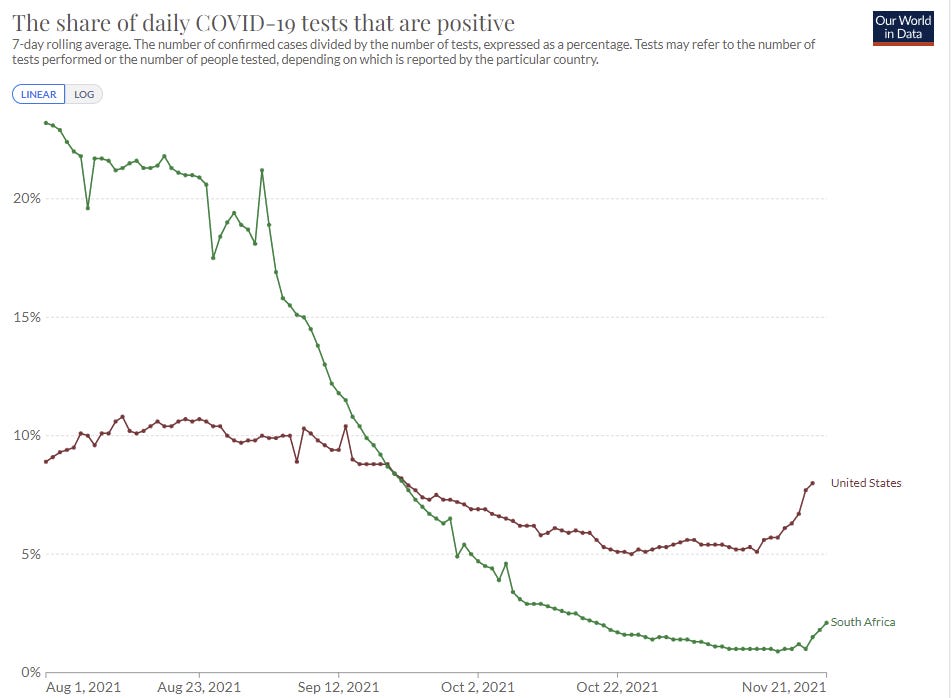
You might think this is lack of testing, but no, it’s not.
This is the biggest reason to think this could all still be a false alarm. A large rise from a very small number means a lot less.
Despite this, of course, it’s still too late to contain the situation, which is why I’m saying that we will basically never contain such situations. A few thousand cases is too many to come back from, and we’re already seeing cases in many other places – one in Belgium, one in Hong Kong and one in Israel.
World Reaction
The financial markets are taking this seriously. You can never be sure about such things, but from what I’ve seen the details of what is moving in what direction sure look like this is the ‘Covid beta’ rather than something else.
The large decline in Crypto is especially interesting, because we saw a similar thing in 2020 that at the time clearly didn’t reflect long term prospects and was based on the flows that happen in such situations. At the time I was too distracted to pull the trigger, which is quite sad. If the current move gets much bigger, then to the extent that one wants to be long, it seems like a potential opportunity to buy cheap (Not Investment Advice!).
That market reaction was motivating to get me to look at this quickly and take it seriously, and is definitely influencing my probability of this being ‘for real’ quite a bit.
The other big response was, of course, travel bans. The WHO warning against them is what got me to snap to attention and write this quickly, which also tells you what I think of the WHO:
I have a lot of news sources, but for pure ‘just the basic things that are happening around the world regarding Covid’ my source of choice is the BNO Newsroom and in particular their twitter feed. Here’s some stuff that happened, in chronological order, after a lot of different news items about various new European case counts and restrictions over the previous few days.

As far as I can tell the WHO’s reaction was to attempt to stop nations from closing borders.
An accompanying press release did a standard call for preventative measures, which doesn’t seem connected to any model of how that would help.





The UK goes first and fast, cutting off travel from six countries rather than only South Africa, as one would do if taking this seriously. Of course, if taking this fully seriously you’d cut off everyone, but that’s a much bigger ask, especially at this early stage. Again, we never actually win at this, we only lose slower.
The note of a ‘threat to the vaccine programme’ looks to me like an important insight into the psychology here. The entire pandemic is seen through the eyes of the vaccinations, and as a fight to be won, rather than as a more broad situation in which vaccines are the strongest tool but the goal is to do the best we can in practice.
So we see the jump, as always, to ‘maybe the vaccines will stop working.’

Israel second. The UK did first doses first and otherwise took its own path to vaccine distribution, some would say even exiting the EU for related reasons. Israel did what it had to do to get more vaccine doses faster, and give them out quickly.
Those two being the first two to ban travel does not seem remotely like a coincidence.

The timeline says this jump came after the UK and Israel took action, which is impressive. The extra day’s data makes a big difference.

Direct link to the tracker here. Doesn’t appear to let you view things over time, so here’s the snapshot now, as I’m writing this, at 12:52pm on 11/26, during which time South Africa’s case count hasn’t been updated:

Singapore up next, and again, does this seem like a coincidence to you at all?

Israel and Hong Kong (and later Belgium) detected the first cases not in Southern Africa, while also seeming like the places that would notice such cases first. Let’s not pretend it hasn’t arrived here yet.

Note the contrast. The EU proposes a ban and will consider it. The UK went ahead and did it.
Not that every EU member was about to sit around and wait.






Germany noting the ‘variant of concern’ and then saying they’re ‘very worried’ while not stopping flights is an interesting news item there, while others drop the hammer. Short Germany?

As long as you don’t, ya know, actually do anything about it, as we’ll see in a second.


Oh well, nothing we can do about things like that.

Very glad to see that they did quarantine the entire flight.

Total failure.


Yes, I believe toast is an appropriate description.


We are still going to ‘wait for more information.’ Others do not have that luxury.

Less than a day still isn’t so bad – they did it while I was writing this. Kudos.

Seriously, WHO, could you people be any less helpful? We all agreed on Nu and now we have to type Omicron all the time? Couldn’t even use Xi?
Here’s their announcement.
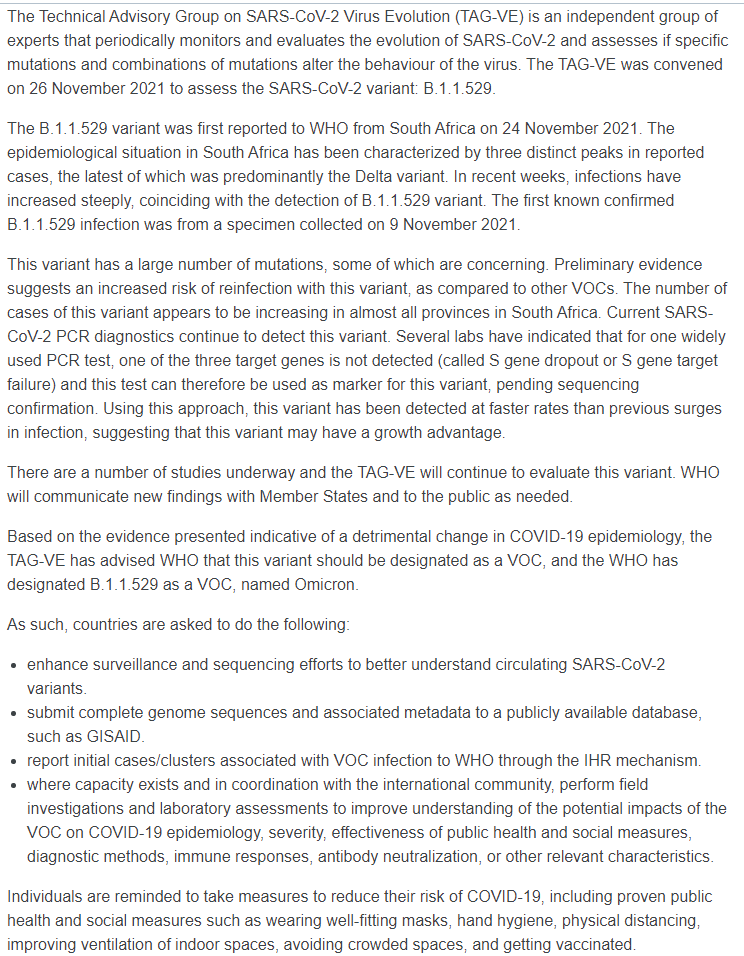
So please gather information and encourage everyone to take all the same measures as before, and otherwise do nothing.
A quick scan of the new Belgian report does not seem to indicate information I didn’t already have from Twitter. Here are its recommendations:
7. Recommendations
The identification of a first B.1.1.529 positive case in Belgium (but also at the European level) highlights the rapid international spread of this variant. Risk mitigation strategies should include travel restrictions or reinforced screening procedures at the international level (not only travels linked to South Africa), accelerating vaccination campaigns worldwide and accelerating the delivery of booster doses for the most fragile populations, reinforcing disease control interventions at all levels. Further, offering maximal support to African countries to ensure reinforced disease surveillance and control remains a high priority. These standard recommendations should shortly be updated based on the evolution of our understanding of the impact of this variant with regard to virulence, infectiousness, vaccine efficacy and activity of existing antivirals.
That all seems highly sensible, if incomplete.
EDIT: The actual moment I hit the send button, we did in fact restrict travel:

Current Model
In the interest of the speed premium, I’m going to summarize my current thinking, while noting that I haven’t had that much time to think it over (nor has anyone else), and that my opinions will doubtless change quickly as the situation develops and also I have time to think.
Also, having to do this gives me a chance to do some intuition pumping.
These numbers are best guesses right now but please don’t take them too seriously or stick to them as the situation changes. If I don’t look stupid with some of these, then that would be me twisting my numbers to not look stupid. These numbers probably don’t live in the same universe and you could probably make very good bets against me by figuring out where they’re inconsistent, were I willing to book them, but these numbers aren’t supposed to be robust enough for that.
Anyway, here goes.
Chance that Omicron has a 100% or bigger transmission advantage in practice versus Delta: 30%.
The estimates in the threads were very large, including numbers like 170% and 500%, but I notice that my median estimate is far lower. That’s because the overall numbers are still small, and variants have a way of starting out spreading super rapidly for various reasons well in excess of how much better they end up spreading at equilibrium. This could all still be very overblown, and especially that’s likely in terms of the huge estimates of transmissibility advantage.
Chance that Omicron will displace Delta: 70%.
This implies there’s about a 40% chance that Omicron will displace Delta but with a <100% advantage, which seems at least reasonable.
In terms of this being a favorite at this point, I agree it’s still early, but also the pattern matching is way, way too good, and there weren’t any false alarms that got to this level of concern.
Chance that Omicron is importantly more virulent than Delta: 25%.
I mean everyone knows they don’t know, and this is definitely me guessing in a largely unprincipled way at this point. The virtue of putting a number on it even when you have no idea.
Chance that Omicron is importantly immune erosive, reducing effectiveness of vaccines and natural immunity: 50%.
There’s a lot of baseline biological reasons to suggest this, and there’s a lot of trust that this translates into actual effects, but will the effect be ‘important’? That’s harder to say, and we have skepticism from previous rounds. Seems likely that protection against infection will decline.
Chance that Omicron means the vaccinated and previously infected are no longer effectively protected against severe disease until they get an Omicron-targeted booster shot: 5%.
I find this much less likely than a waning of immunity to infection and modest decline in severe disease protection. Our immune systems are robust, the protection against severe disease from vaccines and infections has held up even when breakthroughs happen or vaccine effectiveness declines over time. 5% is a lot more worried than I was yesterday! And if that does happen, things are going to go very haywire, but for now I’m only at 5%.
Chance we will be getting boosters modified for Omicron within 6 months of our previous booster shot: 15%.
I notice that I don’t expect this to happen in many of the worlds where it would be an obviously necessary idea.
Chance that Omicron is less vulnerable to non-antibody treatments like Paxlovid or Fluvoxamine: 5%.
This is an ‘unprincipled’ 5% based on weird stuff happening, and I could probably get a lot more confident in a hurry by asking experts quick questions, but as far as I can tell there’s no interaction between such treatments and the changes in Omicron. So I can’t rule it out, but I find this unlikely.
Chance we are broadly looking at a future crisis situation with widely overwhelmed American hospitals, new large American lockdowns and things like that: 20%.
My gut is something like: Even with a huge transmission advantage, we might not get to this point because of vaccinations and Paxlovid, if we have enough time for that, and because every wave ends up peaking on its own one way or another, and there’s a ton of immunity already even if it will be weakened somewhat. If we assume 100% transmission advantage, there should be enough time to get Paxlovid online, so I think this is less likely than the doubled transmission, but I do notice that it’s on the table. Again, I expect to move this number quickly if I were to think more about it.
Final Thoughts
This has been written super quickly, so it will have mistakes, especially mistakes of reasoning. That’s how it works in a rapidly developing situation. Here’s the practical view for now.
- If you haven’t had a booster, I’d consider getting one. Waiting for modifications for Omicron seems wrong, as if that happens demand will exceed supply for too long. If Omicron is for real, it might become very difficult to get an appointment for a while.
- If you have things to do that involve exposure, all the more reason to do them now rather than wait. If you have travel plans a while out, don’t get too attached.
- If you don’t have emergency supplies in case of another lockdown, maybe start thinking about what you’d need and stock up early on things that will keep or would be super important. Even if it’s unlikely, you want to notice when it becomes likely.
- The chances of things ever fully ‘returning to normal’ went down once again, except if we decide to return to normal and live our lives anyway. We need a plan to do that, now more than ever.
- We’ll know more soon.
95 comments
Comments sorted by top scores.
comment by evhub · 2021-11-26T21:28:38.227Z · LW(p) · GW(p)
My guess is it’s actually quite a bit of evidence against any strong potential gains from updating, but weak evidence against weak gains.
So far, all talk of immune escape has mostly been exactly that, talk. That should make us wary of expecting it out of a new variant, or of updating too much from people’s concerns.
If a new variant comes along that does offer substantial escape from the vaccines, we will need to update the vaccines and get new versions out as quickly as possible. Will we be able to do that?
Technologically I have no worries. We’ll have that part solved within the week and probably within one day.
The problem here is original antigenic sin. Once you've been vaccinated against a particular variant, getting another vaccine for a very close relative generally won't do anything other than reactivate the antibodies your body developed the first time around, rather than causing you to develop new antibodies specific to the new variant. Here is a study looking at this in the context of Covid vaccines, which does suggests some things we could do to mitigate the effect, but overall I think you shouldn't expect vaccination against a specific variant to help all that much relative to just getting another wild-type booster.
So, independent of the fact that new, variant-specific vaccines not being produced is evidence that they wouldn't help much, our prior should also be on them not helping much due to original antigenic sin (except for people who have yet to be vaccinated or infected at all). Original antigenic sin is a reason that, if some new variant does come along with significant vaccine escape—but which is still similar enough to the wild-type for original antigenic sin to apply—just developing new, variant-specific vaccines might not actually be an effective way out.
Replies from: Wei_Dai, CraigMichael, Zvi, James_Miller, gabriel-holmes, SDM, oumuamua, JoeBloggs↑ comment by Wei Dai (Wei_Dai) · 2021-11-27T23:18:38.861Z · LW(p) · GW(p)
From your linked paper https://www.cell.com/trends/immunology/fulltext/S1471-4906(21)00177-0:
Experience from the IAV field indicates that multiple serial exposures to variant IAV strains might imprint (focus) the immune response to a narrow array of well-conserved viral epitopes relative to emerging subsequent strains and this might eventually reduce vaccine effectiveness. Randomizing multiple cohorts over time to either serial or partial immunization might also yield important neutralization data, although powering such studies for efficacy would be challenging. Larger observational studies of cohorts receiving serial immunizations might therefore also prove useful.
This suggests that it may be a good idea to avoid getting a booster now (with the ancestral spike protein) and wait for an Omicron-specific booster instead. (Use other precautions to avoid infection in the meantime.)
Replies from: Wei_Dai, JoeBloggs↑ comment by Wei Dai (Wei_Dai) · 2021-12-03T07:56:15.349Z · LW(p) · GW(p)
A trio of vaccine experts made the same point in https://www.washingtonpost.com/outlook/2021/11/29/booster-shots-universal-opinion/:
Although we believe it is likely that the current vaccines will continue to protect against severe disease caused by omicron, the possible need for a booster shot targeting a vaccine-resistant variant could be a reason to hold off for now on a booster targeting the original variant. For one thing, if omicron proves resistant to vaccine-induced protection against serious disease, then a booster dose with the current vaccine may not help. It’s also possible that repeatedly “training” the immune system to fight the original variant could reduce the effectiveness of a variant-specific booster. This phenomenon, called “original antigenic sin,” has been observed with influenza and human papillomavirus vaccines. In other words, for those not in immediate need of a boost, there may be a significant advantage to waiting until a booster more closely aligned with circulating variants becomes available; boosting on the original antigen could be counterproductive.
↑ comment by JoeBloggs · 2021-11-29T19:06:22.580Z · LW(p) · GW(p)
I don't understand why you think that follows from that passage. I interpret it to mean serial exposure to a series of variant-specific vaccines may reduce overall effectiveness. e.g. Imagining a hypothetical variant sequence of V -> V' -> V''. I interpret this as saying if you vaccinate for each with a variant-specific vaccine the effectiveness of the V'' vaccine will be less effective than the original vaccine was for V. Therefore they theorize it may be advantageous to break the chain and e.g. give half the people the V' vaccine when available while the other half skips V' and is given V'' vaccine when available.
Their reasoning isn't entirely clear to me since it's not clear to me exactly how and by what mechanism(s) the vaccine effectiveness may degrade.
↑ comment by CraigMichael · 2021-11-27T06:55:02.141Z · LW(p) · GW(p)
Vaccine is for the S2 subunit. If I’m reading this correctly the subunit is 686–1273 residues. https://www.nature.com/articles/s41401-020-0485-4
I had previously read that delta had one mutation there and the vaccines still held up pretty well. It looks like Wikipedia agrees, and that would be D950N. https://en.wikipedia.org/wiki/SARS-CoV-2_Delta_variant#Mutations
Looking at the 686-1273 mutations for Omicron in the s2 subunit, it looks like there’s a lot more (9 if the article is correct so far) N764K, D796Y, N856K, Q954H, N969K, L981F, V1069I, Δ1265, L1266I https://en.wikipedia.org/wiki/SARS-CoV-2_Omicron_variant#Mutations
So… if the vaccine is for the s2 subunit, and Delta had one s2 change that dropped effectiveness enough for breakthroughs, then eight more s2 changes will probably be a lot worse in terms of dropping vaccine effectiveness.
Are there any biology types that can tell me how accurate/crazy this reasoning is?
Replies from: jowen↑ comment by jow (jowen) · 2021-11-27T22:02:28.131Z · LW(p) · GW(p)
I believe the mRNA vaccines are based on the full-length spike protein, not just the S2 subunit. The S1 subunit includes the critical receptor binding domain, which is a common target of neutralizing antibodies induced by vaccination, and is the location of many further mutations seen in Omicron.
Edit: To be clear, this fact doesn't invalidate your point about the new mutations looking possibly quite bad for vaccine efficacy.
Replies from: CraigMichael↑ comment by CraigMichael · 2021-11-28T02:11:20.989Z · LW(p) · GW(p)
I’m pretty certain on this point as it was related to discussion a few months ago about antibody dependent enhancement. Vaccines targeted the s2 subunit as it was thought to be the least likely to create ADE and also the slowest to mutate. https://www.lesswrong.com/posts/5yarKt4MqRjv72mYv/covid-8-26-full-vaccine-approval?commentId=Dwuyzup535CaGEJ4b [LW(p) · GW(p)]
As quoted in that post:
Replies from: jowenFrom the early stages of COVID-19 vaccine development, scientists sought to target a SARS-CoV-2 protein that was least likely to cause ADE. For example, when they found out that targeting the nucleoprotein of SARS-CoV-2 might cause ADE, they quickly abandoned that approach. The safest route seemed to be targeting the S2 subunit of the spike protein, and they ran with that, wrote Derek Lowe, PhD, in his Science Translational Medicine blog "In the Pipeline."
↑ comment by jow (jowen) · 2021-11-28T03:04:40.115Z · LW(p) · GW(p)
Following your link and looking for the original source, I found that actually Derek Lowe appears not to say that in his blog post, as least not anymore (he made an edit there---though it is not clear that it ever mentioned the S2 subunit).
https://www.science.org/content/blog-post/antibody-dependent-enhancement-and-coronavirus-vaccines
Specifically, it was the vaccines that targeted the N (nucleoprotein) antigen of the coronavirus that had ADE problems,
while the ones that targeted the S (Spike) protein did not. Update: this isn't accurate. There was trouble after immunization with a nucleoprotein-directed vaccine, but ADE could also be seen with some of the Spike-directed vaccine candidates as well - see reviews here, here, and here.
Anyway, it is possible for us to independently see from many different sources that the vaccines code for full-length spike (with minor modification to stabilize the naturally somewhat "floppy" protein in the desired "prefusion" configuration). For example, from here (https://www.nejm.org/doi/full/10.1056/nejmoa2035389):
The mRNA-1273 vaccine is a lipid nanoparticle–encapsulated mRNA-based vaccine that encodes the prefusion stabilized full-length spike protein of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
Also, the S1 subunit is that part that contains the receptor binding domain, and it is possible to read in many papers (e.g. https://www.science.org/doi/10.1126/scitranslmed.abi9915) that the vaccines elicit antibodies that target this domain.
Replies from: CraigMichael↑ comment by CraigMichael · 2021-11-29T07:43:33.423Z · LW(p) · GW(p)
It looks liken you’re right. Thanks for checking here.
↑ comment by Zvi · 2021-11-26T22:12:44.630Z · LW(p) · GW(p)
Presumably we still should have shifted everything over anyway, it's a freeroll that can only help?
Replies from: ChristianKl, evhub↑ comment by ChristianKl · 2021-11-27T10:20:24.075Z · LW(p) · GW(p)
Announcing it might have meant that people who wait to get vaccinated till the new version arrives get better protection which is a message that the people at the CDC hate to tell people.
That might be enough to push the institutions into a state where they won't develop a slightly better vaccine that doesn't add much when it might make people more skeptical of taking the current one?
↑ comment by evhub · 2021-11-26T22:16:01.587Z · LW(p) · GW(p)
Yes, at least that's also my understanding—especially since we are still vaccinating new people, not just giving out boosters. My point is just that it seems like we shouldn't rely on updated vaccines being able to change the course of the pandemic in a major way.
↑ comment by James_Miller · 2021-11-27T01:50:13.237Z · LW(p) · GW(p)
Thanks for providing this, it seems extremely important for trying to predict how the pandemic will play out. So we should have been much more scared of COVID variants than we would be absent original antigentic sin. As it was predictable that COVID, because it was new to humans, would mutate this means those, including myself, who had never heard of this force likely underestimated the expected harm of COVID. Why wasn't this something that the official experts were talking about long ago?
Replies from: Norman Borlaug, ChristianKl↑ comment by Norman Borlaug · 2021-11-28T18:36:49.989Z · LW(p) · GW(p)
Probably for the same reason they downplayed the drop in vaccine efficacy from Delta: they didn't want to increase vaccine hesitancy.
↑ comment by ChristianKl · 2021-11-29T15:05:24.228Z · LW(p) · GW(p)
Why wasn't this something that the official experts were talking about long ago?
We weren't the official experts talking about airborne transmission long ago?
↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-27T02:03:17.879Z · LW(p) · GW(p)
Is original antigenic sin widely accepted? It's not clear to me that there's a strong consensus based on your link.
EDIT:
I did a bit of (not very thorough) googling on original antigenic sin, and managed to convince myself that, yes, it's a thing. But then to help myself sleep I looked up "overcoming original antigenic sin" and came across this:
https://news.emory.edu/stories/2012/08/flu_vaccines_original_sin/campus.html
Adjuvants! I really have no idea what they are, but I seem to remember that these are added to all the covid vaccine?
Replies from: liam-donovan-1↑ comment by Liam Donovan (liam-donovan-1) · 2021-11-27T18:09:03.946Z · LW(p) · GW(p)
My uninformed impression is that an "adjuvant" is just something that stimulates increased immune response, which has historically been an additional chemical (such as an aluminum salt) added to vaccines. The mRNA vaccines do not contain these chemicals, but some people confusingly refer to the lipid nanoparticles that surround and protect the mRNA as adjuvants (because they also help increase immune response). I haven't seen any evidence that these lipid nanoparticles are the kind of adjuvants that might mitigate OAS, but that doesn't mean much because I'm a total nonexpert.
Replies from: Douglas_Knight, cistrane↑ comment by Douglas_Knight · 2021-12-03T18:48:59.851Z · LW(p) · GW(p)
Adjuvants are for activating the immune system to respond to free-floating virus particles. If the virus actually infects a cell and produces proteins on the cell's surface, that is a different signal to the immune system and adjuvants are not needed. Thus adjuvants were not needed for traditional live/attenuated vaccines and 21st century mRNA and vector vaccines (AZ, etc), but were needed for 1980s recombinant protein vaccines (Novavax) and traditional dead/inactivated vaccines.
↑ comment by Sammy Martin (SDM) · 2021-11-27T15:07:30.555Z · LW(p) · GW(p)
How does Original Antigenic Sin work for natural immunity vs vaccine derived immunity? Is it a stronger impediment for one vs the other?
Also, this whole topic seems (I think) to be mostly independent of the T-cell immunity that gives you the baseline immunity to severe disease - the reason for Zvi's low estimate of full immune escape, I think.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-28T12:34:24.537Z · LW(p) · GW(p)
This doesn't directly answer your question but it appears that people who received mRNA vaccines produced fewer antibodies for one of the four endemic coronaviruses than those who were naturally infected. If that's true, it's very encouraging news as far as adapting vaccines is concerned:
https://www.medrxiv.org/content/10.1101/2021.09.30.21264363v1
↑ comment by oumuamua · 2021-11-28T17:35:43.676Z · LW(p) · GW(p)
There's this post, which suggests that Original antigenic sin is unlikely to be a problem. I really hope that's true.
Replies from: Korz, Norman Borlaug, Douglas_Knight↑ comment by Mart_Korz (Korz) · 2021-11-28T20:37:16.043Z · LW(p) · GW(p)
Regarding the link: Possibly you did not activate the markdown editor for your profile?
In that case you can create one by marking the link-text: a hover-menu will appear with the option to add a link
↑ comment by Norman Borlaug · 2021-11-28T18:45:14.839Z · LW(p) · GW(p)
The link is working for me, though the markdown you used isn't formatting the way it is supposed to.
So if I understand correctly, Moderna gave a third dose of either the B.1.351 variant shot or the original 1273 shot to patients and found that those given the B.1.351 shot had higher levels of neutralizing antibodies against the variant?
This seems to suggest that we could do strain specific boosters against COVID. I suspect that would be particularly true for Omicron since it has so much more antigenic drift than the other variants.
↑ comment by Douglas_Knight · 2021-12-03T18:57:19.554Z · LW(p) · GW(p)
An alternate interpretation of the result is that Beta just didn't have much immune escape. That fact that it was crushed by Delta suggests that. The vaccine produced antibodies that were more tuned to Beta than those from the original vaccine, but the difference was slight, just a factor of 2. We won't know about OAS until we have a variant with real immune escape, which may well be Omicron. But I'm not worried about OAS because it's a lower order effect.
↑ comment by JoeBloggs · 2021-11-28T20:53:56.176Z · LW(p) · GW(p)
FWIW, there is other SARS2-specific supporting evidence that immune imprinting may be an issue for vaccine updates. Lately in the UK Health Security Agency weekly vaccine surveillance reports they have begun including this note:
>(iii) recent observations from UK Health Security Agency (UKHSA) surveillance data that N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.
(From page 39 paragraph 3 of https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1036047/Vaccine_surveillance_report_-_week_47.pdf)
The UK tracks seropositivity of S and N antibodies. N antibody positivity is used to track the subset of people who were previously infected. This note implies the immune system may not be updating its response when challenged with a new variant of the live virus.
comment by rossry · 2021-11-27T02:06:48.188Z · LW(p) · GW(p)
I give the WHO kudos for picking omicron instead of nu. (Actually, I'm pretty shocked that they did something this common-sensical, and notice that I am surprised.) I spent Friday morning (= Thursday evening, US time) talking out loud with colleagues about the new nu variant and after like two attempts to clarify what the f--- I actually meant, multiple people independently joked that it was so bad we should just skip nu and go to omicron.
If you've only ever discussed it in text, you're underestimating how bad it is to use "nu" as an adjective in verbal conversation.
Replies from: charbel-raphael-segerie, Mark_↑ comment by Charbel-Raphaël (charbel-raphael-segerie) · 2021-11-28T08:39:56.932Z · LW(p) · GW(p)
Just curious, what's the problem with "nu" in verbal conversation ?
Replies from: jimv, rossry↑ comment by jimv · 2021-11-28T10:07:05.065Z · LW(p) · GW(p)
It sounds like "new".
I imagine conversations going like: "So, this nu variant, huh?" "Which new variant? We're getting minor variations all the time." "But the nu one..."
And that would get even trickier if you want to some newer new variant that succeeds this one.
"Wait, when you say [?new | ?nu], are you talking about the old nu variant or the new new variant?"
comment by Tamay Besiroglu (tamay-besiroglu) · 2021-11-27T19:16:31.334Z · LW(p) · GW(p)
Thanks for writing this, I found it useful.
> Chance that Omicron will displace Delta: 70%.
I think this is a little overconfident given my read on the currently available evidence. There have also been a dozen or so instances when new variants dominated some country that subsequently fizzled out and never went global (either because a fitter variant emerged shortly after or because it turned out to be less infectious than was initially thought). Since I called you out last time [LW · GW] on being overconfident ex-post, let me try doing it ex-ante this time.
I'd be willing to offer 1:2 odds (e.g. my $100 against your $200) that Omicron will not be found in more than 50% of sequences in the US according to Covariants.org any day before and including March 1st 2022. Note, I'd want to reserve the right to change the terms if you accept later than 48 hours from when this comment was posted (if/when the situation becomes clearer).
↑ comment by Zvi · 2021-11-28T00:55:02.348Z · LW(p) · GW(p)
66% by March 1 is very close to 70% eventually, and I noted my confidence level is low, but I will consider if I become more confident within the window. Thank you for the offer, in any case.
What is your fair? 50%? 30%?
Replies from: tamay-besiroglu↑ comment by Tamay Besiroglu (tamay-besiroglu) · 2021-11-29T12:58:25.118Z · LW(p) · GW(p)
Got it. My fair is probably at around 50% right now.
Replies from: Zvi↑ comment by TheMajor · 2021-11-28T01:08:58.356Z · LW(p) · GW(p)
There have also been a dozen or so instances when new variants dominated some country that subsequently fizzled out
I completely failed to notice this, whoops. Do you have some more information on this?
Replies from: tamay-besiroglu↑ comment by Tamay Besiroglu (tamay-besiroglu) · 2021-11-28T11:40:23.490Z · LW(p) · GW(p)
Yea. Gamma was the dominant strain in Brazill, Luxembourg, Chile, Argentina, and a few other places in early-to-mid 2021, but never become the dominant strain in the US. Similarly for Lambda in Peru, Mu in Colombia, 20B/S:732A in Mexico, 20A/S:439K in Slovenia, 20E in Lithuania, and a handful of other strains in some other countries. This is all from Covariants.org. Many of these countries do roughly as much sequencing as SA does, so it seems like an appropriate reference class for thinking about Omicron.
Replies from: neel-nanda-1↑ comment by Neel Nanda (neel-nanda-1) · 2021-11-28T13:55:07.425Z · LW(p) · GW(p)
What fraction of these fizzled out because they were displaced by a fitter variant vs just not spreading further? That seems very important for figuring out how much to freak out
Replies from: tamay-besiroglu↑ comment by Tamay Besiroglu (tamay-besiroglu) · 2021-11-29T12:56:13.936Z · LW(p) · GW(p)
To be clear, I'm not proposing a bet that no newly emerging variants are going to be consequential. I'm interesting in making a much narrower claim about the global reach of Omicron.
↑ comment by Norman Borlaug · 2021-11-28T19:30:15.880Z · LW(p) · GW(p)
That website covariants.org is amazing. I've been looking for something like that for so long.
comment by TropicalFruit · 2021-11-28T04:50:09.061Z · LW(p) · GW(p)
Me:
- Sees news stories about Omicron popping up
- I wonder if Zvi's written a breakdown yet?
- Checks LW
- Zvi published on Nov 26
Zvi, you're an absolute legend. Thanks for getting these out so fast. If it weren't for your write-ups, I have no idea where I would go for anything even remotely resembling a minimally biased, rational review of the current evidence.
comment by Mitchell_Porter · 2021-11-27T04:24:04.882Z · LW(p) · GW(p)
Before we speculate on how Omicron may spread, perhaps we should do a postmortem on Delta? In India, after the big spike of April, the daily new cases dropped way down. In pre-Omicron South Africa, daily new cases were also low. Presumably there are other countries where a Delta boom has died away to a trickle of daily cases. Do we have any understanding of why?
About Omicron, there is speculation that it has been selected to escape vaccines. But my understanding was that vaccines don't do much to stop the spread anyway, they just protect against severe illness. Is this wrong? Or is the idea that people who do fall ill, produce enough extra virus, that there is selection pressure to produce a virus which evades even the protection against illness?
I'll also remark that natural immunity is likely to be more robust than mRNA-vaccine-derived immunity, since the latter gives you antibodies just against the spike protein, while natural immunity will produce antibodies against other components of the virus too.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-28T12:29:57.006Z · LW(p) · GW(p)
It seems that Omicron may have mutated over time within a single immunocompromised host, so it's not clear to me how natural selection applies.
Replies from: rudi-c↑ comment by Rudi C (rudi-c) · 2021-11-28T23:06:15.179Z · LW(p) · GW(p)
Sources?
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-30T16:46:35.555Z · LW(p) · GW(p)
"Another possibility, still speculative but discussed by many scientists in recent days, is that omicron evolved over many months within an immunocompromised patient with a protracted infection. In a patient treated with therapeutics such as monoclonal antibodies or convalescent sera, a viral strain that can survive the assault can potentially amass a host of mutations. Such cases have been documented, but they are not known to have led to outbreaks in the general population."
Source:
https://www.washingtonpost.com/health/2021/11/29/how-bad-is-omicron-variant/
This does seem to be a recurring theme - very slow mutation for the most part, and lots of new mutations occurring in immunocompromised "supermutators".
comment by gilch · 2021-11-26T20:46:11.125Z · LW(p) · GW(p)
Seriously, WHO, could you people be any less helpful? We all agreed on Omicron and now we have to type Omicron all the time? Couldn’t even use Xi?
Replaced "Nu" one too many times?
Replies from: ejacob, Zvi↑ comment by ejacob · 2021-11-27T04:05:53.124Z · LW(p) · GW(p)
I estimate a 900% chance that no variant will ever be named 'Xi' as it would link it to a certain head of state.
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-27T07:33:08.249Z · LW(p) · GW(p)
I dunno, it's pronounced "Kai" (rhymes with "guy") but you might be right
Replies from: jimv↑ comment by jimv · 2021-11-27T08:32:49.923Z · LW(p) · GW(p)
No, the letter between nu and omicron is pronounced something like 'ksai'. https://en.m.wikipedia.org/wiki/Xi_(letter)
The one you're probably thinking of is later in the Greek alphabet. https://en.m.wikipedia.org/wiki/Chi_(letter)
comment by Norman Borlaug · 2021-11-28T19:27:18.523Z · LW(p) · GW(p)
I think you are likely underweighting the possibility that Omicron could significantly decrease vaccine efficacy.
Omicron has 50 mutations including 30 in the spike protein. I believe Delta had 9. https://twitter.com/EricTopol/status/1464410605402480641
https://twitter.com/MichaelWorobey/status/1464325657861574659
"The B.1.1.529 (omicron) Spike looks a whole lot like a 'polymutant' Spike experimentally generated to evade antibody responses from infection or vaccination, as noted by @theodora_nyc
And at long last, here's the tweet I read two days ago and have been looking for ever since. https://twitter.com/theodora_nyc/status/1464257411582148608
> "I wish I was as optimistic @jbloom_lab Our polymutant spike has 20 aa substitutions and is almost completely resistant to neutralization by almost all vaccinated and convalescent plasma we tested. This new one has more in overlapping regions."
I don't have a great method for estimating exactly how effective existing vaccines will be against symptomatic infection but I'd give 95% odds they perform worse against Omicran than Delta. If I had to give a point estimate, I'd guess that your protection against symptomatic infection by this variant from being triple vaxxed will be 40%. But my error bars are very wide: a 95% confidence interval from 10% protection to 90%.
On a side note: it's pretty scary to me that scientists are running experiments where they mutate coronaviruses to specically evade vaccines. Haven't we learned our lesson here from the experiments that were going on in Wuhan? Even if the lab leak theory turns out to be false (which is looking less likely every month), it's very clear that these experiments have tremendous potential to do harm. Why are we still doing this? It just seems totally nuts to me.
I'm going to put on my tinfoil hat here for a second: what are the odds that Omicron was created by a lab doing experiments on SARS-CoV-2? I keep going back to that tweet from Michael Woroby:
> "The B.1.1.529 (omicron) Spike looks a whole lot like a 'polymutant' Spike experimentally generated to evade antibody responses from infection or vaccination"
If the spike looks a lot like one that was experimentally generated to evade antibody responses, what are the odds that Omicron was created through such experiments? How many labs are doing the types of experiments that are being done at Theodora's lab? If the number is high enough it seems likely that there will be a leak at some point given what we know about the history of such incidents at even the highest BSL facilities. Anyone have thoughts about how to more rigorously constrain the odds that this variant was accidentally released from a lab doing gain of function research?
↑ comment by Richard_Kennaway · 2021-11-28T20:58:48.067Z · LW(p) · GW(p)
"The B.1.1.529 (omicron) Spike looks a whole lot like a 'polymutant' Spike experimentally generated to evade antibody responses from infection or vaccination"
At this point I have to wonder about the existence of antinatalist virologists.
↑ comment by jow (jowen) · 2021-11-29T01:57:49.089Z · LW(p) · GW(p)
If the spike looks a lot like one that was experimentally generated to evade antibody responses, what are the odds that Omicron was created through such experiments?
The research in question seems to be described in this Nature paper, where the authors say (emphasis mine):
To more precisely map the targets of polyclonal neutralizing antibodies in individuals who are convalescent, we passaged a recombinant vesicular stomatitis virus (rVSV)/SARS-CoV-2 chimeric virus1,5 in the presence of each of the RU27 plasmas for up to six passages. rVSV/SARS-CoV-2 mimics the neutralization properties of SARS-CoV-2 (refs. 1,5) but obviates the safety concerns that would accompany such studies with authentic SARS-CoV-2.
So, regarding safety, it seems the place to start would be understanding the properties of this rVSV/SARS-CoV-2 construct. Further details are here.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-11-29T15:13:44.959Z · LW(p) · GW(p)
To me the most remarkable thing about the Nature paper is that the word biosafety or BSL doesn't appear in it.
Saying they obviated the need of safety concerns and then doing the experiments without any biosafety protocols seems crazy.
↑ comment by henryaj · 2021-11-28T23:57:41.746Z · LW(p) · GW(p)
Do you know what kind of research Theodora's lab is actually doing? (She doesn't have a surname on Twitter so I can't find her). But I imagine research into spike protein mutants could just involve synthesising spike protein that has mutations and assaying the binding affinity of antibodies to the synthetic spike protein – not necessarily creating mutated viruses.
(undergrad biochemistry was a long time ago. I could well be wrong)
↑ comment by TAG · 2021-11-28T21:31:35.311Z · LW(p) · GW(p)
“The B.1.1.529 (omicron) Spike looks a whole lot like a ‘polymutant’ Spike experimentally generated to evade antibody responses from infection or vaccination”
If the spike looks a lot like one that was experimentally generated to evade antibody responses, what are the odds that Omicron was created through such experiments?
Alternatively, gain of function research is useful and gives us advanced warning of natural mutations. I don't know if that is the one true narrative , but I'm not ruling it out.
Replies from: Norman Borlaug, ChristianKl↑ comment by Norman Borlaug · 2021-11-29T14:45:30.400Z · LW(p) · GW(p)
That's certainly the argument its proponents make, and perhaps it's true in some circumstances. But after looking at some of the research grants made to the Wuhan Institute of Virology in the years leading up to the outbreak, it's clear to me that there really is dangerous research out there whose theoretical benefits are vastly outweighed by the costs.
For example, there was some really dangerous gain-of-function research happening in a BSL-2 facility, which are just not designed to contain dangerous pathogens.
But we inherently need international agreements to deal with these problems. I believe the US banning gain of function research in 2015 was one of the driving factors that pushed the research overseas into Wuhan.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-11-29T14:56:19.640Z · LW(p) · GW(p)
But we inherently need international agreements to deal with these problems. I believe the US banning gain of function research in 2015 was one of the driving factors that pushed the research overseas into Wuhan.
That seems doubtful to me. It seems to me like as part of wanting world class scientists this is something the Chinese wanted regardless of US research policy as long as the research is held at high esteem by the international scientific community.
↑ comment by ChristianKl · 2021-11-29T14:58:16.249Z · LW(p) · GW(p)
Alternatively, gain of function research is useful and gives us advanced warning of natural mutations.
Even if it would produce useful information, that might still be the case that Omicron exists for those reasons. It's strange to use the word alternatively hear when any information gained doesn't negate the cost of potentially producing variants like Omicron.
To the extend that you believe that there's useful information, can you give any example of anything useful coming out of it?
Replies from: TAG↑ comment by TAG · 2021-11-29T16:50:38.790Z · LW(p) · GW(p)
If you want to determine the balance of evidence, by all means do so, but you can't do that by completely disregarding the alternative explanation.
There was a time when thus place was all about the avoidance of bias.
Replies from: ChristianKl↑ comment by ChristianKl · 2021-11-29T22:07:19.254Z · LW(p) · GW(p)
Whether or not something provides valuable information is orthogonal from it being dangerous. The two aren't alternatives. Something can be valuable&dangerous.
Replies from: TAGcomment by yanky · 2021-11-26T22:23:52.688Z · LW(p) · GW(p)
"When the WHO warned against travel restrictions, that’s when I knew in my gut what we were dealing with."
This comes across as conspiratorial, and frankly anti-bayesian. Do you mean to say that if the WHO had not warned against travel restrictions, or promoted travel restrictions you wouldve take that as a good sign?
comment by Lukas_Gloor · 2021-11-26T21:30:07.928Z · LW(p) · GW(p)
The Belgian woman developing symptoms 11 days after coming back from Egypt suggests that the disease timeline is substantially longer than with Delta. This makes me think immunity escape plays a very big factor in how it was able to outcompete Delta this quickly in South Africa. (But obviously there could also be a missing piece or misinformation in the Egypt-Belgium story.)
Replies from: Zvi, siclabomines↑ comment by Zvi · 2021-11-26T22:11:00.436Z · LW(p) · GW(p)
I have to assume the 11 day delay is unusual, or even that perhaps that case didn't actually come from Egypt. If it usually took 11 days then there's no way it grows this fast (and if it still does, seriously, it's time to give up.)
Replies from: dawangy↑ comment by dawangy · 2021-11-26T23:50:22.459Z · LW(p) · GW(p)
11 days could be unusual based on the Hong Kong report:
Based on the report it seems that someone arriving Nov 11 had enough virus to test positive by Nov 13, and the person he infected had enough virus to test positive on Nov 18. Both were sent to the hospital but it is unclear whether this was part of a standard procedure or if they were ill enough to need to go.
Replies from: rossry↑ comment by rossry · 2021-11-27T01:58:31.861Z · LW(p) · GW(p)
Both were sent to the hospital but it is unclear whether this was part of a standard procedure or if they were ill enough to need to go.
Testing positive was sufficient to get them sent to the hospital, and they had mandatory PCR testing every ~3 days; this is no evidence about their symptoms.
(I recently went through HK arrival quarantine -- in the same hotel, no less -- and researched the operating procedure runbook out of personal interest.)
Replies from: dawangy↑ comment by siclabomines · 2021-11-27T19:12:14.431Z · LW(p) · GW(p)
Why does it follow that a longer time to develop symptoms suggests immune escape?
Also, if the timeline is longer, then the estimates of how much more transmissible Omicron is, based on the time it's taken for it to displace Delta, should be even greater, right?
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2021-11-28T11:46:13.042Z · LW(p) · GW(p)
The speed by which Omicron outcompeted Delta is explained by three broad contributors:
- Generation time
- Immunity escape
- Transmissibility in susceptible populations
We learn (probabilistically) that the first factor isn't lower than in Delta, and may even be higher (longer generation time). This leaves even more work to be done for the other two factors. You're right that in theory, Omicron could just be crazy good at spreading in susceptible populations. However, I think that's unlikely on priors given that you get an easy 3x increase in overall transmissibility with full immune escape, and that seems easier, mutation-wise, than the virus suddenly turning into something that's a lot more transmissible than any coronavirus we've ever seen.
↑ comment by siclabomines · 2021-11-28T17:58:45.890Z · LW(p) · GW(p)
Makes sense to me...
On the other hand, if it takes longer to show symptoms but it's still equally transmissible since early but for longer, you get higher Rs without surprising new mechanisms of transmission. Also, it may also be escaping our current precautions instead of the immunity.
comment by Sammy Martin (SDM) · 2021-11-27T15:16:58.435Z · LW(p) · GW(p)
Israel second. The UK did first doses first and otherwise took its own path to vaccine distribution, some would say even exiting the EU for related reasons. Israel did what it had to do to get more vaccine doses faster, and give them out quickly.
Those two being the first two to ban travel does not seem remotely like a coincidence.
You could add that the UK ran essentially all the big clinical trials that discovered useful treatments, aside from those personally funded by Tyler Cowen. There's an interesting and important discussion to be had on this topic at some future point - especially as to how these decision-making procedures got off the ground in the first place. I wrote a short summary of that here [EA(p) · GW(p)].
The large decline in Crypto is especially interesting, because we saw a similar thing in 2020 that at the time clearly didn’t reflect long term prospects and was based on the flows that happen in such situations. At the time I was too distracted to pull the trigger, which is quite sad. If the current move gets much bigger, then to the extent that one wants to be long, it seems like a potential opportunity to buy cheap (Not Investment Advice!).
Further in the realm of Not Investment Advice, I considered (but didn't) shorting global markets when the Omicron news came out, and in the process of dithering the decline had already started. If some of the extreme high estimates (500%?!) in this thread are true then the decline we've seen so far looks like an under-reaction, but it's not clear to me that there's enough info to make a safe bet on that. A lot of trading ideas got floated in discussions about previous variants, but didn't result in any firm consensus that I can recall (other than the short-selling that happened for original covid)
comment by devansh (dpandey) · 2021-11-26T22:12:06.109Z · LW(p) · GW(p)
Until new information comes out which clarifies the infectivity and severity of Omicron, especially against the vaccinated, I'm potentially more worried about outsized and concerning responses to the new variant than I am about Omicron itself. To be clear, this isn't diminishing the potential bad results of Omicron—but in terms of actual infectivity and severity, I don't expect it to be a lot worse than Delta. Vaccine resistance is more concerning, especially considering original antigenic sin.
That being said, my school (and California) has been requiring masking throughout the pandemic, and we closed schools for more than a year. I'm deeply concerned about the potential mental health effects of going back to virtual school, both on myself and people I care about. The current masking requirements for (even 80+ percent vaccinated) schools being more stringent than the masking requirements for basically anything else, including bars, is absolutely ridiculous to me. This is only going to get worse, as parents in my district will do absolutely anything to make sure their whims are satisfied. I'm fairly confident that if Omicron looks to be a general threat, regardless of its actual danger to students, they will close en masse.
I think your model is largely accurate, and the only one I would disagree with is the last—where I'd put the chances, considering vaccines. Paxlovid. and Fluvoxamine, as <10%. I'd add one final chance at ~40% that schools from kindergarten to colleges widely close for >3 months.
Replies from: edward-pascal↑ comment by Edward Pascal (edward-pascal) · 2021-11-27T21:45:35.051Z · LW(p) · GW(p)
I worry sometimes about burnout effects. What if we do all that and Omikron isn't so bad, but two variants further down the road is 'the one' and no one is willing to do anything about it?
Replies from: gabriel-holmes↑ comment by tkpwaeub (gabriel-holmes) · 2021-11-28T14:56:43.353Z · LW(p) · GW(p)
Good point - "boy who cried wolf" syndrome
comment by gjm · 2021-11-28T12:25:08.260Z · LW(p) · GW(p)
The Times of India claims that the chairwoman of the South African Medical Association claims that Omicron is producing only "mild disease". There are lots of ways for that to turn out to be wrong, but if it's true it might be very good news: a new variant that's infectious enough to take over quickly and that does hardly any damage when it infects you.
comment by Lukas Finnveden (Lanrian) · 2021-11-27T10:39:06.542Z · LW(p) · GW(p)
I think this final graph is a bit confused here, unless ‘the original strain’ here means Delta. Delta had about a 120% advantage over ‘the original strain’ or 70% over Alpha. I’m going to take this to mean 500% as compared to that 120%, so 600% of original versus 220% of original, or about a 170% additional increase. Which is… better, but still quite a lot.
I'm pretty sure the graph is trying to say 500% over delta. If you run the numbers [LW(p) · GW(p)] on a very similar graph, you get that the new disease is slightly above 5.5 times as infectious as delta, which you could round to a 500% increase. (Assuming identical generation length. Also, I haven't looked into sources for the numbers.)
South Africa’s vaccination rate is sufficiently low, and this rate of spread so high, that it wouldn’t much matter if there was vaccine escape properties, although it would presumably matter if there was escape from natural immunity.
I don't know why you expect a large difference there. I'd guess that [LW(p) · GW(p)] roughly equal numbers of people in south africa has been vaccinated as has natural immunity.
Or, okay, I can see two reasons to expect natural immunity to be a bigger deal:
- natural immunity is more common in the most exposed part of the population.
- there's more uncertainty about the amount of natural immunity in south africa, and if south africa has very sizeable natural immunity and there's substantial immunity erosion, that would be a pretty good explainer for why omicron would be spreading so much faster than delta. So there's some bayesian update towards south africa having sizeable natural immunity.
Don't know where this nets out.
Replies from: TurnTrout↑ comment by TurnTrout · 2021-11-27T17:10:01.967Z · LW(p) · GW(p)
5x Delta transmissibility seems insane. I... Don't have gears level models which prohibit such a thing, but wouldn't that give it a reproduction rate between 25 and 45?! Even chickenpox is only 12.
Replies from: Lanrian↑ comment by Lukas Finnveden (Lanrian) · 2021-11-27T17:34:31.829Z · LW(p) · GW(p)
A factor 1.5-3 of that could be immune erosion, in which case the R0 would be more like 10-20. And more importantly, I don't know anything that contradicts Zvi's intuition that this little data shouldn't push us far away from our priors.
comment by tkpwaeub (gabriel-holmes) · 2021-11-28T11:21:48.026Z · LW(p) · GW(p)
Looks like Australia just found cases of Omicron:
comment by LatticeDefect · 2021-11-27T13:37:07.215Z · LW(p) · GW(p)
What updates on your predictions, if any, would you make if we learned that the variant developed from a long-term infection in an immunocompromised person, i.e. had plenty of opportunity to adapt to the immune response.
comment by ZachWeems · 2021-11-27T08:46:01.338Z · LW(p) · GW(p)
Omicron has the same spike protein deletion as Alpha. This deletion causes a strong 'SGTF' signal in certain PCR tests. Back when we were most concerned about Alpha, the company Helix made a page that showed what percentage of their PCR's had SGTF by date & state. Only enough data to use for CA, TX, and FL, but much more up-to-date than sequencing data.
The page seems to be deleted for now, but here is a link the company's Twitter. I expect at some point they'll announce they're doing the same thing again. https://twitter.com/my_helix
Replies from: ZachWeemscomment by Annapurna (jorge-velez) · 2021-11-26T19:36:55.569Z · LW(p) · GW(p)
Re: effectiveness of Paxlovid vs Omicron:
https://twitter.com/MonicaGandhi9/status/1464099757408751616?t=_ewDKnnijBgpeAzydqew4g&s=19&fbclid=IwAR2Jmkxy_iLjXkQhUoGrtBqMimpqBTWy5NLPRWheemNWcJAcT6j93JjydWA
↑ comment by CraigMichael · 2021-11-27T07:03:50.471Z · LW(p) · GW(p)
Thanks for this. But had to copy and paste. Hopefully LW makes this a hyperlink- https://twitter.com/MonicaGandhi9/status/1464099757408751616?s=20
comment by TropicalFruit · 2021-11-28T04:54:06.181Z · LW(p) · GW(p)
I love how one of the paragraphs in here is essentially:
"Buy bitcoin, not investment advice."
In all seriousness, though, what makes you believe you have an edge over the market, when it comes to the crypto crash due to Omicron? Everyone in the market is trying to price in the risk of Omicron, why do you think you can do it better?
I certainly believe Omicron poses essentially zero risk to bitcoin, and so if the market is pricing in such a risk, I'd like to buy, but is it actually justified to believe my appropriation of the risk is more accurate than the market's as a whole?
Would you mind clearly articulating where you think your edge is?
Replies from: MondSemmel↑ comment by MondSemmel · 2021-11-28T16:36:00.500Z · LW(p) · GW(p)
I'm not sure whether this answers your question, but Zvi is an MTG Hall of Famer and knows some stuff about risk. (There's also some overlap between MTG progamers and Poker players.) And separately, he's working in the crypto space (on a trading card game called Emergents), so he's not clueless about the domain.
Apart from that, "efficient markets" is a strong argument, but not a slam-dunk one.
And finally, these are just his initial musings based on very early information, so even if one thought they had an edge here, they'd still have to think hard about whether acting earlier but with less reliable information was better than waiting for better information.
EDIT: To be clear, I have no clue about investing in cryptocurrency.
comment by Steven Byrnes (steve2152) · 2021-11-28T04:28:41.152Z · LW(p) · GW(p)
I'm surprised that you of all people didn't mention population inhomogeneity ... There's a most-exposed tier of the population (based on work situation, living situation, etc.), and by now everyone in that tier has (mostly natural) immunity. An immune-escaping variant would spread rapidly within that subpopulation, right?
Replies from: TheMajor↑ comment by TheMajor · 2021-11-28T10:08:55.236Z · LW(p) · GW(p)
This seems correct to me, but I don't immediately see the importance/relevancy of this? At any rate the escape is speculative at this point.
Replies from: steve2152↑ comment by Steven Byrnes (steve2152) · 2021-11-28T11:38:00.202Z · LW(p) · GW(p)
Oh, I was responding to this part:
We should presume that if something takes over quickly, it has a very large advantage infecting people who are unvaccinated and lack natural immunity.
We should presume that if it also has an additional property of vaccine escape, that seems like quite a coincidence, so it seems unlikely.
We should consider this even more unlikely if the variant started out in places with low vaccination rates.
I'm suggesting that population inhomogeneity weakens this argument, and that immune escape + population inhomogeneity would seem to be a plausible explanation of how omicron appears so much more infectious than delta. I wasn't assuming immune escape / erosion, I was arguing for it being more likely / less unlikely given what we know.
comment by SuperDaveWhite (superdavewhite) · 2021-11-27T19:27:51.718Z · LW(p) · GW(p)
“In an unlikely but conceivable turn of events, what if that scientist becomes infected with the virus, which leads to an outbreak and ultimately triggers a pandemic?” Fauci wrote in a paper reported on by The Australian. “Scientists working in this field might say — as indeed I have said — that the benefits of such experiments and the resulting knowledge outweigh the risks.” National Institute of Allergy and Infectious Diseases (NIAID) Director Anthony Fauci defended “gain-of-function” research in 2012
comment by Cedar (xida-ren) · 2022-04-03T20:47:58.162Z · LW(p) · GW(p)
One thing notably missing from this post is the analysis about severity and how different countermeasures can make the virus evolve in different ways. E.g. if we stop people with fevers from travelling, it would give a no-fever variant a lot of advantage over a fever -causing variant.