March Coronavirus Open Thread
post by Elizabeth (pktechgirl) · 2020-03-08T22:45:07.348Z · LW · GW · 378 commentsContents
378 comments
This thread was created on 3/8/2020, or approximately one million years ago in virus time. It’s getting pretty bloated now, and a lot of things that were high value at the time have been eclipsed by events, making karma not a very useful sorting tool. So I’m declaring this thread finished, and asking everyone to move over to the April Coronavirus Open Thread [LW · GW].
Interested in what happened in this thread? Here’s the timeless or not-yet-eclipsed highlights:
- Scott Alexander comes up with [LW(p) · GW(p)] Hammer and Dance 6 days before Tomas Pueyo
- Spiracular on why SARS-Cov-2 is unlikely [LW(p) · GW(p)] to be lab-created.
- Two documents collating estimates of basic epidemiological parameters, in response to this thread [LW(p) · GW(p)]
- Discussion [LW(p) · GW(p)] on whether the tuberculosis vaccine provides protection against COVID-19.
- Suggestive evidence [LW(p) · GW(p)] that COVID-19 removes sense of taste and smell.
- Could [LW(p) · GW(p)]copper tape be net harmful?
378 comments
Comments sorted by top scores.
comment by Scott Alexander (Yvain) · 2020-03-14T03:41:04.817Z · LW(p) · GW(p)
China is following a strategy of shutting down everything and getting R0 as low as possible. This works well in the short term, but they either have to keep everything shut down forever, or risk the whole thing starting over again.
UK is following a strategy of shutting down only the highest-risk people, and letting the infection burn itself out. It's a permanent solution, but it's going to be really awful for a while as the hospitals overload and many people die from lack of hospital care.
What about a strategy in between these two? Shut everything down, then gradually unshut down a little bit at a time. Your goal is to "surf" the border of the number of cases your medical system can handle at any given time (maybe this would mean an R0 of 1?) Any more cases, and you tighten quarantine; any fewer cases, and you relax it. If you're really organized, you can say things like "This is the month for people with last names A - F to go out and get the coronavirus". That way you never get extra mortality from the medical system being overloaded, but you do eventually get herd immunity and the ability to return to normalcy.
This would be sacrificing a certain number of lives, so you'd only want to do it if you were sure that you couldn't make the virus disappear entirely, and sure that there wasn't going to be vaccine or something in a few months that would solve the problem, but it seems like more long-term thinking than anything I've heard so far.
I've never heard of anyone trying anything like this before, but maybe there's never been a relevant situation before.
↑ comment by AlexSchell · 2020-03-14T11:28:29.937Z · LW(p) · GW(p)
If you first do lockdowns to get new cases to ~0 and then relax, optimistically you will get localized epidemics that you can contain with widespread testing, contact tracing, and distancing if needed. Cost of testing & tracing and having to do occasional local/regional lockdowns could end up being manageable until treatment/vaccine arrives.
My main reason for optimism is Korea's and China's success containing a large outbreak. We will be expecting the secondary epidemics and reacting quickly, so they will be small when detected, so should be much easier to contain than the first surprise outbreak.
We'll get data on this in the coming months as China loosens restrictions. There is option value in containing asap and first trying things other than deliberate infections.
Replies from: jackson-l↑ comment by Jackson L (jackson-l) · 2020-03-19T17:39:07.878Z · LW(p) · GW(p)
Linking the The Imperial College paper here (which a lot of people have referenced lately) that addresses these two approaches: (a) mitigation, which focuses on slowing but not necessarily stopping epidemic spread –reducing peak healthcare demand while protecting those most at risk of severe disease from infection, and (b) suppression, which aims to reverse epidemic growth, reducing case numbers to low levels and maintaining that situation indefinitely. (https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf)
The biggest issue with the suppression strategy is the time required for the lockdown - until R reaches low enough levels that eliminate human-to-human transmission, or until a vaccine is available. Estimated 12-18 months with a r0 of 2.4.
In fact the more successful a strategy is at temporary suppression (China), the larger the later epidemic if the lockdown is lifted prematurely - due to lesser build-up of herd immunity (Figure 3, "post-September 2020").
Mitigation: "In the most effective mitigation strategy examined, which leads to a single, relatively short epidemic, the surge limits for both general ward and ICU beds would be exceeded by at least 8-fold under the more optimistic scenario for critical care requirements that we examined. In addition, even if all patients were able to be treated, we predict there would still be in the order of 250,000 deaths in GB, and 1.1-1.2 million in the US."
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-19T16:25:56.414Z · LW(p) · GW(p)
Their paper is not relevant as they do not analyze testing & contact tracing AT ALL, only mentioning it briefly in the Discussion section. I think everyone who thinks the strategy I describe might be feasible (which now seems to be most informed participants in the discussion on here & rationalist Twitter) more or less agrees with the Ferguson analysis if you assume you can't do testing & tracing & isolation or they won't work.
Replies from: jackson-l↑ comment by Jackson L (jackson-l) · 2020-03-19T23:14:12.411Z · LW(p) · GW(p)
Yes you are correct, succinctly addressed here " They ignore standard Contact Tracing [2] allowing isolation of infected prior to symptoms. They also ignore door-to-door monitoring to identify cases with symptoms [3]. Their conclusions that there will be resurgent outbreaks are wrong. After a few weeks of lockdown almost all infectious people are identified and their contacts are isolated prior to symptoms and cannot infect others [4]. " https://necsi.edu/review-of-ferguson-et-al-impact-of-non-pharmaceutical-interventions
↑ comment by gwillen · 2020-03-14T03:57:48.115Z · LW(p) · GW(p)
I've spent some time thinking about endgames here. (Not that I feel like I've come to any conclusions. I wish I knew what e.g. the WHO thought the endgame was.) The biggest problem I see with this idea is the lag between input and output -- when you change your quarantine measures, you can't observe the result for at least the 5-7 days it takes the newly infected to get symptoms, and longer if you want to get a lot of confidence in your measurement, over the noise inherent in the system.
Control systems with high lag like this are incredibly difficult to work with. Especially in the presence of exponential growth like this system has -- if you accidentally let R get a bit too high, it will be a week or two before you notice, and in that time you will have seeded a ton of cases that you will have to track down and deal with.
I think the most hopeful endgame here, near-mid-term, is that we find a combination of antivirals with high effectiveness against COVID-19, which reduces the rate of severe pneumonia dramatically. At that point our hardest constraint, ventilators, will get relaxed. Beds are a lot easier to deal with a shortage of.
Mid-long-term, of course, we're all hoping for a vaccine. Who knows whether that's going to happen.
In Singapore, and China-outside-Hubei, my impression is that very aggressive high-bandwidth contact tracing is working effectively. Unfortunately, at least Seattle has already given up on that, as far as I can tell. But if we can simultaneously raise our ability to do contact tracing effectively, and lower the value of R below 1 until we get the number of cases under some kind of control, we ought to be able to use a combination of contact tracing and more moderate measures to keep it there. I hope.
Of course, the organization primarily responsible for contact tracing in the US is currently rather indisposed. But in theory, the states should be just as able to do it, although some scaling up may be in order.
Replies from: Roko↑ comment by Roko · 2020-03-19T10:46:42.163Z · LW(p) · GW(p)
Control systems with high lag like this are incredibly difficult to work with. Especially in the presence of exponential growth like this system has -- if you accidentally let R get a bit too high, it will be a week or two before you notice, and in that time you will have seeded a ton of cases that you will have to track down and deal with.
This is why you need to have borders on multiple scales and cancellation of large events.
If one case slips through, in a week or two they will infect a handful of new people. If you have set up a system of regional and national borders, as well as cancelled large events, you will find out about this trace the contacts and temporarily increase the strength of the lockdown in only that region.
This strategy nearly worked in South Korea, but then patient 31 was a superspreader:
https://graphics.reuters.com/CHINA-HEALTH-SOUTHKOREA-CLUSTERS/0100B5G33SB/index.html
↑ comment by Alexander Gietelink Oldenziel (alexander-gietelink-oldenziel) · 2020-03-20T12:36:02.722Z · LW(p) · GW(p)
Just like to chime in to say that this (=' flattening the curve/ herd immunity') fundamentally doesn't work, and you don't need to have a PhD in epidemiology from Imperial College to understand this [but you might need a PhD in epidemiology to misunderstand it], just basic arithmetic and common sense.
Suppose 50% of the UK (33 million people) get the virus of which 5% (~ 1.8 million people) will need serious hospitalization [conservative estimate]. The current capacity of ICU beds in the UK is something on the order of 2000 beds , depending on occupancy rates, ability to scale up et cetera. Let's be extremely optimistic and somehow the UK is able to quintuple this capacity [as far as I can tell this is unlikely]. When somebody is sick they might need care for 2 weeks. The annual hospital capacity is: 25 weeks * 10.000 beds= 250k. At the moment the capacity is nowhere that (perhaps 50-100k).
You can see that 1.8 million is far larger than 100k or even 250 k. Even wildly optimistic estimates will not yield anything realistic. This assumes that the government is somehow able to control the infection spreading over a year; instead of two months. There is no reason to think they can do this without extreme (partial) lockdown measures. Controlling the R0 is extremely hard. All the mild measures seem to help only a tiny little bit. If the R0 is only a bit over 1, we still have exponential growth; and you have merely pushed timelines back a few months.
Can we perhaps expose young people but lock up older people for one-two years [when the vaccin might arrive]? I find this is extremely unlikely; you need only a couple people to flout the rules to wipe out an entire nursing home.
Is it worth it to (partially) lock down the entire country for a year to save maybe a hundred thousand old people?
There are only two real possible approaches:
1. Let the Boomers die. If we're lucky the death rate is ~0.7 percent. When (not if) hospitals overflow this will easily triple. Without medical care, once you go critical you simply can't breath [though I heard something to the effect that most/many deaths are due to cardiac arrest]. Simple as that. With a massive host population the virus will mutate and we might have the same problem every year [<- this very real possibility is perhaps the most important to think about].
2. total lock down -> squash the curve, followup with massive testing Gangnam style and extensive contact tracing [also: Fast-track all possible vaccins/treatments and fire Chief Medical Officer]. This seems to work so far in all East-Asian countries. Why the people with actual experience and succes in this matter get systematically ignored in these discussion will be a question for historians.
I know my preferred approach. There is no linear response to an exponential tide.
[1] https://www.telegraph.co.uk/global-health/science-and-disease/huge-regional-differences-intensive-care-bed-numbers-threaten/
↑ comment by Roko · 2020-03-20T19:30:13.554Z · LW(p) · GW(p)
I agree with this analysis completely.
There is a strategy bifurcation: Either you lock down hard and contain/eradicate, or you just accept the losses and tell people to go on as normal, with isolation of the vulnerable.
The middle path is not favorable. You take both the human damage and the economic damage.
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-18T02:18:14.478Z · LW(p) · GW(p)
The South Korean approach seems to be roughly as effective as the Chinese approach but significantly less costly and disruptive. SK managed to halt exponential growth and currently cases are increasing linearly at a rate of 75 or so per day. This has been achieved without lockdowns or extensive border closings. Instead, the key ingredient appears to be rapid, extensive and largely free testing, and an educational campaign that stresses the importance of hand washing and staying at home.
↑ comment by Raemon · 2020-03-14T06:38:24.969Z · LW(p) · GW(p)
China is following a strategy of shutting down everything and getting R0 as low as possible. This works well in the short term, but they either have to keep everything shut down forever, or risk the whole thing starting over again.
UK is following a strategy of shutting down only the highest-risk people, and letting the infection burn itself out. It's a permanent solution, but it's going to be really awful for a while as the hospitals overload and many people die from lack of hospital care.
I'm confused about why the second strategy works better than the first strategy at killing it permanently. If you shut down everything, shouldn't everything die out faster? (Unless you have open borders and let it in again, but wouldn't that also apply in the UK case?)
Replies from: gwillen↑ comment by gwillen · 2020-03-14T07:23:55.343Z · LW(p) · GW(p)
The first strategy leaves you with a huge population of people with no immunity to the virus, which means you have to keep holding the lid on it indefinitely or you're back to square one.
In the second strategy, everyone ends up either immune or dead, which doesn't mean the virus is gone -- it will remain endemic -- but there will be no giant flood of new cases when people resume their lives.
(Obviously it's not quite as simple as that if the virus doesn't generate durable immunity. Then you end up with something like the flu, where partial immunity keeps it vaguely tamped down with occasional flares.)
Replies from: willbradshaw↑ comment by willbradshaw · 2020-03-15T08:40:43.631Z · LW(p) · GW(p)
Clarification: you don't need everyone to be immune or dead. Just enough people that the remaining population can't sustain a continuous epidemic.
Replies from: gwillen↑ comment by gwillen · 2020-03-15T22:04:39.153Z · LW(p) · GW(p)
Right, yes, agreed and good point -- my understanding is that a naive epidemiological model gives a fraction of 1 - (1/R_0) of the population needing to be infected, to drive the effective value of R (new transmissions per infected person) below 1, at which point the population can no longer sustain epidemic spread.
↑ comment by Lukas Finnveden (Lanrian) · 2020-03-16T21:12:42.331Z · LW(p) · GW(p)
Isn't this exactly what "flatten the curve" is about? Because a lot of people are talking about that as a solution, including some governments.
The main problem is that the curve needs to get really flat for hospitals to have time with everyone. Depending on how overwhelmed you want your hospitals to be, you could be in lock-down for several years. Some calculations in this article.
↑ comment by Mmv · 2020-03-16T21:52:12.127Z · LW(p) · GW(p)
Isn't "social distancing" the in-between strategy already? I was thinking of something similar today, when questioned whether to have a friend to my house. If I followed the strictest measures, I wouldn't. But then, if nobody did and we were essentially on self-quarantine mode, then the virus wouldn't spread at all or very, very, little and we would be hovering in small numbers for months, until next fall/winter, when it could get really risky again (presuming that weather has an influence, like with flu). So doesn't the social distancing strategy want some appreciable degree of transmission, high enough to get to herd immunity in a reasonable amount of time, but slow enough to avoid a hospital crisis? Are governments just relying on the idea that some people will ignore the suggestions, and we'll get a reasonable degree of transmission over time during social distancing?
↑ comment by Liam Donovan (liam-donovan-1) · 2020-03-15T08:53:43.285Z · LW(p) · GW(p)
Your goal is to "surf" the border of the number of cases your medical system can handle at any given time (maybe this would mean an R0 of 1?) Any more cases, and you tighten quarantine; any fewer cases, and you relax it. If you're really organized, you can say things like "This is the month for people with last names A - F to go out and get the coronavirus". That way you never get extra mortality from the medical system being overloaded, but you do eventually get herd immunity and the ability to return to normalcy.
I'm pretty sure that's exactly what the UK is trying to do? I'm actually pretty confident that the UK government isn't planning to have " hospitals overload and many people die from lack of hospital care. ". Even if they were sure that was the best approach (and they just didn't think of your idea?) it would be completely unfeasible politically
↑ comment by syllogism · 2020-03-14T21:24:33.190Z · LW(p) · GW(p)
But why can't we eradicate the virus? Let's say China shuts down international travel, keeps doing what they're doing, and then slowly eases back up in some area, letting the people in that city comingle and go back to work, but still restricting travel in and out. Let's say they get that city back running, with no coronavirus cases after a month.
At the same time...Won't they also have basically eradicated other influenza there? Even if not entirely, there should be much less cold and flu, right? So as soon as coronavirus creeps back in, it should be much easier to contain.
I guess my thinking here is, if coronavirus is much more virulent than the flu, and this type of containment works to almost eliminate the coronavirus, could China...actually eradicate the flu, at the same time? If not, why not?
The problem comes in from other countries. If China goes to all this effort and the US, Europe, UK etc don't, do we would end up with this weird hazmat curtain? Asian countries would join China in eradicating the disease, and Australia and New Zealand would probably join them.
Replies from: gwillen↑ comment by gwillen · 2020-03-16T00:28:48.195Z · LW(p) · GW(p)
I've already heard that influenza cases are down in countries that enforced social distancing / lockdowns for coronavirus. However, it really only takes one country not doing this for influenza to return to typical incidence -- there's no real reason to believe it will be eradicated. (However, the same seems true for COVID-19, so I'm not sure what to expect there.)
Replies from: syllogism↑ comment by syllogism · 2020-03-16T02:09:48.066Z · LW(p) · GW(p)
I agree that actually eradicating influenza feels far-fetched. But on the other hand, it's quite a lot easier to work with than COVID-19. Influenza isn't nearly as infectious, most people have immunity, and it's barely transmissible at all when the carrier is asymptomatic.
Imagine you actually did have the "hazmat curtain" situation. Everyone is asked to take their temperature on the way in, and significant fines (and potential visa cancellations) are imposed if you lie. At first nearly everyone is checked to verify, but this is relaxed to spot-checks as people get used to never breaking the rule. Few enough people are getting sick that when people do report influenza symptoms, they can be tested, and contact tracing can be employed to halt the outbreak and trace it back to how it was introduced.
If there are no animal reservoirs for the disease, I think that could be viable? It's expensive, but influenza is a big cost in itself, in lost productivity and other problems.
The big problem I see for eradicating coronavirus will be in poorer countries --- Africa, the middle east, etc. The outbreaks there are still pretty small, but there's no real resources to address them, so the problem could grow there until it's really hard to fix.
comment by Pablo (Pablo_Stafforini) · 2020-03-12T23:05:25.858Z · LW(p) · GW(p)
Update: the positions are now filled. See here for the official announcement.
Help wanted: pandemic.metaculus.com project lead
The high interest and proliferation of questions on the novel coronavirus calls for dedicated attention, which led to the formation of pandemic.metaculus.com. Managing it, though, is straining Metaculus's very limited staff and community moderator team. Contingent on acquisition of funding (which Metaculus is working to secure), Metaculus is looking to bring onboard someone to help manage this project. Components would include:
- Managing the pandemic site and question series as a sort of "editor in chief" working with the community moderators (as Tamay does now for Metaculus in general.)
- Helping build data products and analyses out of the questions and results.
The above indicates a range of skills including pretty strong understanding of Metaculus, and data analysis capability. Science background would be great, and huge bonus for actual medical knowledge. This is probably a part-time role but full-ish time is also imaginable depending upon the person, the duration, and funding.
If you're interested, please send a note and CV to jobs@metaculus.com.
comment by jimrandomh · 2020-03-09T06:52:57.832Z · LW(p) · GW(p)
If this news article is accurate, masks will not be scarce for much longer. That article claims that China is now producing masks at 116M/day, a 12x increase compared to the start of February (5 weeks ago), and that they will export them. This is in addition to mask production in other countries.
I am not sure whether, when combined with production in other countries, this satisfies the entire world demand. But masks aren't complicated objects and aren't made of scarce materials, and this is pretty strong evidence that production can be scaled up even further, if necessary.
In a few weeks, a number of public figures may find themselves doing an awkward about-face from "masks don't work and no one should wear them" to "masks do work and they are mandatory".
(If you are able to buy masks for less than $1/each through ordinary channels, it means the shortage has abated, and you can buy them without worrying about depriving health care workers of those supplies, but you shouldn't stock up on more than you need in the short term until the price has been low for at least a few weeks.)
Replies from: jacobjacob, agc↑ comment by Bird Concept (jacobjacob) · 2020-04-02T23:27:19.126Z · LW(p) · GW(p)
In a few weeks, a number of public figures may find themselves doing an awkward about-face from "masks don't work and no one should wear them" to "masks do work and they are mandatory".
I want to record and reward how this prediction seems to be correct: https://www.washingtonpost.com/health/2020/04/02/coronavirus-facemasks-policyreversal/
↑ comment by agc · 2020-03-09T15:43:18.186Z · LW(p) · GW(p)
I wonder if China will direct the masks to politically friendly countries, or let the free marker decide.
Replies from: andrea-mulazzani↑ comment by Emiya (andrea-mulazzani) · 2020-03-11T13:07:40.814Z · LW(p) · GW(p)
They'd likely ship them out to everyone as fast as they can, this is their chance to regain political points after this disaster. They already helped out Italy by donating medical supplies and enough people on the social medias are starting to regard them with a better opinion than other European countries, so as a political move is hugely effective.
Replies from: jmh↑ comment by jmh · 2020-03-12T18:07:22.737Z · LW(p) · GW(p)
I would think that would be the smart thing and the right thing. I suspect it also the thing they will do.
That said, they have also already publicly stated (reported a few days back) they will offer that type of support "for those participating in their belt and road" initiative and I didn't notice (but did not read closely) if they mentioned nonparticipating countries and where they would stand.
Might be more about prioritization in the line.
comment by jimrandomh · 2020-03-09T06:49:36.379Z · LW(p) · GW(p)
I heard a rumor of someone in the Bay area claiming to work in the intelligence community, to be terminally ill, and to have received an experimental COVID-19 vaccine. I think this rumor is false with respect to the specific person, but do note that "military officers with preexisting terminal illnesses who volunteer" is a group that may actually exist, and that at least one drug company claims to have shipped vaccines for a phase 1 trial on Feb 24.
This raises the question: if you're well resourced, desperate, competent, and in possession of expendable military volunteers, how long does development for a vaccine actually take?
Given a candidate vaccine, you need to do three things: find out if confers immunity (and how much immunity), find out if it causes side effects severe enough to not be worth it, and scale up production.
All three of these can be done in parallel. If you have expendable volunteers, you don't need to start with an animal model; you can just give them the vaccine, and see whether they suffer side effects. Testing efficacy can be done in parallel, with the same volunteers, and takes about three weeks--you give the vaccine, wait a week, expose to virus, then wait in quarantine for two weeks.
If you're unlucky, this kills all the test subjects. If you're average-lucky, your test subjects get COVID-19 and die at the same rate as people die of that. If you're lucky, you have solid evidence of effectiveness and moderate evidence of safety. Not as much evidence of safety as you want, and certainly not up to the FDA's traditional standards, but good enough that medical workers in affected areas would seriously consider it.
Maybe it's optimistic, but in my model of the world, there are islands of competence within the intelligence community which do things like this. In most worlds, this project fails, and the public never hears about it. The President, on the other hand, does hear about it. He hears about many vaccine projects with different timelines and different chances of success, and they all blend together. He says on the news that a vaccine will be ready in several weeks, and everyone--the NIAID, the press, the public--mocks him for the mistake, because they don't know about the secret trial. Or maybe he never heard of anything like that, and is just confused; this is not something we are likely to ever know.
Coronavirus could spread unabated, or it could be killed by quarantines, or it could spread but lose its lethality to a new treatment, or we could be surprised by an unprecedentedly fast vaccine. Let us retain our flexibility, and keep our prediction confidence intervals wide.
Replies from: ady-jade-beacham, adamzerner, ChristianKl, Original_Seeing, eternaltraveler↑ comment by Ŀady Jade Beacham (ady-jade-beacham) · 2020-03-09T19:01:44.834Z · LW(p) · GW(p)
Maybe it's optimistic, but in my model of the world, there are islands of competence within the intelligence community which do things like this.
For me, that fits my model of what the US intelligence agencies used to do during the cold war times, and we have unclassified documents about proactive, unethical experimentation they did - like Operation Sea Spray and MK Ultra. I don't know if the 2020 US intelligence community is up to the same task. I get the impression that capability and competence have fallen there, although it's hard to know since so much is classified. But judging by the fact that we have had several elections disrupted by pretty predictable cyberattacks without visible countermeasures, my estimation of their competence has fallen.
On the other hand, here's an article about a UK laboratory infecting people with a non-covid coronavirus to help with vaccine research.
↑ comment by Adam Zerner (adamzerner) · 2020-03-10T01:30:53.917Z · LW(p) · GW(p)
But the space of possible vaccines is very large, I assume. So even with a ton of human testing that only takes three weeks, maybe this still doesn't help much?
Replies from: jimrandomh↑ comment by jimrandomh · 2020-03-10T04:00:41.191Z · LW(p) · GW(p)
In principle, with enough resources, multiple vaccines could be tested this way in parallel. Not that there are that many vaccine candidates to try, as far as I know; but if there were some software that bulk-generated candidate molecules, it could be done, in principle. The limiting input is mobilized resources, not time.
Replies from: ChristianKl, adamzerner↑ comment by ChristianKl · 2020-03-10T15:31:51.494Z · LW(p) · GW(p)
We have the genome of the virus. All the surface proteins of the virus are candidate molecules.
↑ comment by Adam Zerner (adamzerner) · 2020-03-10T06:21:42.208Z · LW(p) · GW(p)
Yeah, if you could reduce the space of possible vaccines to a smaller set of plausible ones, that certainly makes sense.
This makes me wonder, why not just let people volunteer to test risky treatments in general? Because there'd be bad actors who try weird shit willy nilly and misrepresent it to people as more plausible than it really is, such that the harm done to people outweighs the advancements in knowledge? But what if you remove the profit motive and only give this power to government researchers? Would they have too many career-y incentives to be too aggressive?
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-10T15:25:09.766Z · LW(p) · GW(p)
Human trials are much more expensive then trials in mice. If you can already rule out a drug by giving it to mice you save a lot of money that you don't have to invest into your trial with humans.
Replies from: adamzerner↑ comment by Adam Zerner (adamzerner) · 2020-03-10T16:13:19.243Z · LW(p) · GW(p)
True. The downside would be that animal testing is slower, which is I think why jimrandomh was proposing human testing.
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-10T21:26:50.906Z · LW(p) · GW(p)
Speed is not an important variable for government researchers outside of a situation like this where you need a fast response to a pandemic.
Speed matters a bit more for big pharma where it matters if you have one additional year of patent protection for your drug if you develop a year faster but even there the cost tradeoffs are in favor of doing animal testing.
↑ comment by ChristianKl · 2020-03-09T19:14:06.193Z · LW(p) · GW(p)
It seems to me much more likely that the Chinese are doing human trials that skip animal testing then that the US intelligence community does that.
Terminally ill patients don't make good subjects for clinical trials. If you run such a project outside of the reach of the FDA, it seems like a slight against the FDA. It's not a step in which companies that produce vaccines and that want to have good relationships with the FDA want to make.
On the other hand the Chinese government has plenty of people in their prisons that they consider expandable and willing to sacrifice for the greater good. They should also have less institutional resistance to it
Replies from: jimrandomh↑ comment by jimrandomh · 2020-03-09T21:07:55.705Z · LW(p) · GW(p)
The "terminally ill" bit was part of the (probably false) rumor that I heard. Preexisting illness definitely screws with the safety-testing aspect, but there are also illnesses don't interfere with the efficacy testing. I agree that a competent agency uses healthy people for this if they could. If experimenting on healthy people wasn't possible or worth it, one possibility would be to do an efficacy trial on unhealthy people and a safety study on animals in parallel.
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-10T15:26:28.099Z · LW(p) · GW(p)
I have the impression that you ignore the institutional issues that are at play. The intelligence community can't simply deploy a vaccine on their own. They need buy in from the FDA.
Replies from: jimrandomh↑ comment by jimrandomh · 2020-03-10T18:37:00.496Z · LW(p) · GW(p)
Legally speak, yes they would. Practically speaking, however, the FDA has no enforcement power over secret programs in the intelligence community.
I think a lot of people are seriously overestimating the FDA's actual power, and that's causing pretty severe problems. Consider for example this tweet (and a long series like it) by the mayor of NYC, begging the FDA for approvals. While there is no legal precedent to refer to, it's extremely implausible that the FDA could ever get or enforce a judgment of the city of New York for actions taken during a state of emergency, when the FDA itself caused that emergency with culpable negligence.
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-10T19:14:41.887Z · LW(p) · GW(p)
The FDA has no power to stop the intelligence community running tests on patients but they do have the power to declare the results of the tests as not being enough to prove the resulting vaccines safe.
Do you really think that you have a better idea of the institutional power of the various players then the mayor of NYC? The FDA has a lot of relationships that allow it to exert power that are distinct from direct legal tools.
↑ comment by Original_Seeing · 2020-03-12T17:22:18.076Z · LW(p) · GW(p)
There are some articles today about people trying out a drug called remdesivir
↑ comment by eternaltraveler · 2020-03-16T06:01:23.008Z · LW(p) · GW(p)
In general vaccines are very easy to make. You grow the virus you want to vaccinate against, kill or weaken it, and inject it, often with an adjuvant. Viral illnesses that don't have vaccines today are the exception where it turns out that doesn't work and it's more challenging. These difficult ones are what all vaccine research today is focused on, so people think making vaccines is hard.
It usually isn't. Small pox, measles, mumps, rubella, chicken pox, and polio are all gone. Flu is 4 new viruses we make brand new vaccines for every year.
comment by Matthew Barnett (matthew-barnett) · 2020-03-13T21:59:35.595Z · LW(p) · GW(p)
Are the economic forecasts still too sunny?
(Warning: Long comment)
Two weeks ago Wei Dai released his financial statement [LW(p) · GW(p)] on his bet that the coronavirus would negatively impact the stock market. Since then (at the time of writing) the S&P has dropped another 9%. This move has been considered by [LW · GW] many [LW · GW] to be definitive evidence against the efficient market hypothesis, given that the epistemic situation with respect to the coronavirus has apparently not changed much in weeks (at least to a first approximation).
One hypothesis for why the stock market reacted as it did seems to be that people are failing to take exponential growth of the virus into account, and thus make overly optimistic predictions. This parallels Ray Kurzweil's observations of how people view technological progress,
When people think of a future period, they intuitively assume that the current rate of progress will continue for future periods. However, careful consideration of the pace of technology shows that the rate of progress is not constant, but it is human nature to adapt to the changing pace, so the intuitive view is that the pace will continue at the current rate. [...] From the mathematician’s perspective, a primary reason for this is that an exponential curve approximates a straight line when viewed for a brief duration.
The idea that smart investors don't understand exponential curves is absurd on its face, so another hypothesis is that people were afraid to "ring the alarm bell" about the virus, since no one else was ringing it at the time.
Determining which of the above hypotheses is true is important for determining whether you expect the market to continue declining. To see why, consider that if the "alarm bell" hypothesis was true, you might expect that now that the alarm bell has been set off, you now have no epistemic advantage over the market. The efficient market is thus reset. Nonetheless, the alarm bell might be a gradient, and therefore it could be that more people have yet to ring it. And of course both hypotheses might have some grain of truth.
Now that the market has dropped another 9%, the question on every investor's mind is, will it drop further? Yet, if the efficient market has really been debunked, then answering this question should be doable -- and I minimally attempt to do so here.
The approach I take in this post is to analyze the working assumptions of the most recent economic forecasts I could find, ie. try to determine what conditions they expect, which lead to their predictions. If I find these working assumptions to underestimate the virus' impact based on my best estimates, then I conclude, very tentatively, that the forecast is still too sunny. Otherwise, I conclude that the alarm bell has been rung. Overall, there are no fast and easy conclusions here.
The main issue is that this crisis has unfolded far too quickly for many up-to-date forecasts to come out. Still, I find a few that may help in my inquiry.
Disclaimer: I am in no position to offer specific financial advice to anyone, and I write this post for informational purposes only. I have no expertise in finance, and I am not creating this post to be authoritative. Please do not cite this post as proof that everyone should do some action X.
My Parameters
I offer the following predictions about particular parameters of the virus. I admit that many of my parameters are probably wrong. But at the same time, I make a stronger claim that no one else really has a much better idea of what they are talking about. Of course, I gladly welcome people to critique my estimates here.
- I expect that the coronavirus will infect at least a few hundred million people by 1/1/2022. However, I think that as the virus progresses, people will take it very seriously, which implies that the reproduction constant probably won't be high enough for 70 - 80% of the population to be infected. I doubt that countries like the United States will be able to replicate the success at containment found in China, though I'm open to changing my mind here.
- I expect the infection fatality rate (a nonstandard term that means dividing the estimated number of people infected by the number of deaths caused by the virus) to be around 0.7 to 1 percent, with significant uncertainty in both directions. (That said, a paper that was released in the Lancet yesterday says the true figure is probably closer to 5.6% and could be as high as 20%. The sheer insanity of such a prediction should give you an idea of how uncertain this whole thing still is.)
- I expect the virus to temporarily peak in late April or May, but probably return in the winter and do a lot more relative damage given the cold weather.
- I expect hospitals in every major country to be overwhelmed at some point. This will cause the number of deaths to rise, making the 1 percent an underestimate of the true risk. My current (wildly speculative) guess is the true number is 2 percent in untreated populations.
- I expect that a vaccine will not be widespread by 1/1/2021, though I do expect one by 10/1/2021.
- I expect that some sort of anti-viral will be available by this winter, somewhat dampening the impact of the virus when it hits full force. Though it has yet to be seen whether anti-virals will be effective.
- I expect pretty much every country to implement measures like Italy is right now at some point, with the exception of countries with poor infrastructure that cannot manage such a quarantine.
I welcome people to view the estimates from Metaculus, which are more optimistic on some of these parameters than I am. So obviously, take the following analyses with a grain of salt.
Note: throughout this article I use the terms infection fatality rate, case fatality rate, and mortality rate somewhat interchangeably, and at times I do not know whether the author means something different by them. Some people often make careful distinctions between these terms, but it appears most people don't. Therefore, it's really difficult to understand what these analyses are actually saying at times.
JP Morgan
In the last 24 hours, JP Morgan announced that
The US economy could shrink by 2% in the first quarter and 3% in the second, JPMorgan projected, while the eurozone economy could contract by 1.8% and 3.3% in the same periods.
Their prediction is based on their research concerning the coronavirus, compiled here. In many ways, their estimates are quite similar to mine, and they share my sense that this virus will be long-lasting and painful. But in other ways they seem too optimistic. Here are some points,
- At one point they criticize the UK Government's apparent estimate of 100,000 predicted deaths, by saying "To arrive at such an outcome, we had to assume that 38% of the entire UK population is infected (i.e., similar to the 1918 Spanish flu), and that 40% of infected people get sick and then experience 1% mortality; or we had to assume that only 10% of infected people get sick but then experience 4.4% mortality that’s equal to the epicenter of the virus outbreak in Wuhan. Even after accounting for Chinese infection/death underreporting and the difficulty Western countries might have replicating what China has done (the largest lockdown/ quarantine in the history of the world, accomplished via AI, big data and different privacy rules8 ), both of our modeled UK outcomes would be magnitudes worse than what’s occurring in China and South Korea."
- They concur with my vaccine and anti-viral timelines, "While the fastest timeline for vaccines to reach patients is generally 12-18 months, (i.e., Massachusettsbased Moderna’s mRNA vaccine), COVID-19 treatments could possibly become available later this year"
- They cite the fall of H1N1's mortality rate estimate (seemingly) as reason to think that this coronavirus will follow the same pattern, "Early estimates in the fall of 2009 from the WHO3 pegged the H1N1 mortality rate at 1.0%-1.3%, since they were dividing (d) by (c). Four years later, a study from the WHO and the Imperial College of London4 estimated H1N1 mortality as a function of total infections, including both the asymptomatic and the sick. Their revised H1N1 mortality rate using (b) as a denominator: just 0.02%."
My opinion
Whoever wrote this report has done a ton of research, and makes some very intelligent points. It think it would be unfair to say that intelligent investors from JP Morgan "don't understand exponential growth."
That said, I differ significantly in my estimate of whether the UK Government's estimate is valid, and whether the mortality rate will fall just as H1N1 did. The author seemed to be saying that the mortality rate can safely be only be calculated as a fraction of those who got sick with severe symptoms, rather than the total infected population. This fact makes me think that they are underestimating the infection fatality rate.
Moody's Analytics
On March 4th Moody's Analytics released a forecast of economic growth conditioned on the coronavirus becoming a pandemic, which at the time they considered to have only a 35% chance of occurring. Even though this report is somewhat old now, I still include it because this was their 'worst case' report. Their conclusion was that,
Under the pandemic scenario, the global economy suffers a recession during the first three quarters of 2020. Real GDP decreases by almost 2 percentage points peak to trough and declines for 2020 [...] The U.S. economy contracts in all four quarters of 2020 in the pandemic scenario, with real GDP falling by approximately 1.5 percentage points peak to trough and the unemployment rate rising by 175 basis points. The struggling manufacturing, transportation, agriculture and energy industries are hit hard, but so too are the travel and tourism industries and the construction trades. However, there are significant layoffs across nearly all industries, with healthcare and government being the notable exceptions.
The modeling assumption was that "millions" would be infected, and that it would peak by March or April.
Under our alternative Global Pandemic scenario, we expect that there are ultimately millions of infections across the globe, including in Europe and the U.S. COVID-19’s mortality rate is assumed to be 2%-3%, consistent with the experience so far, and a similar percentage of those infected become so sick they need some form of hospitalization. The peak of the pandemic is assumed to occur in March and April, winding down quickly by this summer, with a vaccine in place before next winter.
My opinion
While I find their estimate of the mortality rate to be rather high, this consideration is swamped by the fact that they only think it will infect "millions" of people (which I take to be perhaps 5 - 10 million) worldwide, and the fact that they think we will have a vaccine by next winter. I think Moody's Analytics are seriously low-balling this virus.
This report is probably the best evidence that investors still aren't taking the virus seriously. However, given that this report is about 9 days old though, I think that conclusions from this report should be interpreted with caution.
Capital Economics
A report from Capital Economics came out in the last few days, however, I've been unable to find the exact report. Instead, I can quote media article such as this one, and this one. They report,
Capital Economics also cut its estimate for gross domestic product in 2020, saying the economy would expand just 0.6% instead of 1.8% as previously forecast. [...] Many economists have downgraded their growth forecasts for the second quarter and beyond, but the Capital Economics call is the most pessimistic one yet.
So apparently they expect positive growth for the year, and yet this is one of the most pessimistic predictions from economists? That is striking on its own.
Capital Economics predicts a rebound in 2021 on the assumption that strict social distancing works to contain the coronavirus epidemic.
“If such measures helped to stem the spread of the virus ... they may reduce the risk of a worse-case scenario, in which one-third of the population become infected resulting in a prolonged recession,” Hunter said.
[...]
"We think this is going to have a very significant impact on activity over the next few months," said Andrew Hunter senior U.S. economist at Capital Economics.
[..]
However, Hunter expressed hope that if the number of coronavirus cases in the U.S. peaked in the tens of thousands, then the U.S. economy could "start to recover reasonably quickly."
It's not clear whether their "tens of thousands" in the US is a best case or median case scenario.
My opinion
It's hard to get a real sense of what Capital Economics expects, but the article itself gives the impression that we can still contain the effects, and things will wrap up in a few months. But given that they also mention that billions of people could be infected, it's hard to tell whether they are over or underestimating. I don't have a strong opinion here.
United Kingdom report
On March 11, the United Kingdom released a (long) report on their economic forecast, taking into account the expected impact from the coronavirus. Unfortunately their report did not include the latest figures from the coronavirus, and therefore it's hard to tell whether they are underestimating things.
As set out below, we agreed to close the pre-measures forecasts for the economy and public finances on 18 and 25 February respectively, to provide a stable base against which to assess the impact of the large Budget package. This was before the spread of the coronavirus was expected to have a significant effect on economic activity outside China. As discussed in the document, the outlook is therefore likely to be significantly less favourable than this central forecast suggests – especially in the short term – but to a degree that remains highly uncertain even now.
RaboResearch
A firm called RaboResearch released a forecast on March 12th. They are relatively optimistic,
The coronavirus outbreak has led us to reduce our growth projection for the global economy to 1.6% y/y in 2020
However, their assumptions appear to diverge substantially from mine
Whether we will see a similar spread in other Eurozone member states as we have seen in Italy still remains in doubt – and for now we are not yet assuming that as a base scenario.
In their "ugly" scenario, which they consider unlikely,
would see the virus continue to rage in China, spread to ASEAN, Australia and New Zealand, and the cluster of cases in the US and Europe snowball at an exponential growth rate from their currently low base. In other words, developed economies would also be hit.
Unfortunately, they don't include any actual numbers, so it's hard to tell how bad their ugly scenario actually is. Their absolute worst case scenario, which they call "the unthinkable" also contains no facts or figures,
This scenario is very short. The virus spreads globally and also mutates, with its transmissibility increasing and its lethality increasing too. The numbers infected would skyrocket, as would casualties. We could be looking at a global pandemic, and at scenarios more akin to dystopian Hollywood films than the realms of economic analysis. Let’s all pray it does not come to pass and just remains a very fat tail risk.
Note that I did not bold global pandemic. That was their emphasis.
My opinion
Given that their "unthinkable" scenario describes a global pandemic, which the WHO has already declared, I find it hard to believe that this firm has a clear idea of the economic effects of the coronavirus. Their vagueness makes me think that they are not using solid models of the virus, but instead unsubstantiated intuition, and that they are probably underestimating the impact.
Media reports
According to this investopedia article, the top three stock market news websites are MarketWatch, Bloomberg, and Reuters. Due to the paywall on Bloomberg I only accessed MarketWatch and Reuters. Therefore, I have taken the time to open each of these websites, read the first article that I can see that seems to include both an economic forecast and some type of prediction about a parameter of the coronavirus. To be honest, I wasn't able to find anything really specific. Nonetheless, here are some quotes I found,
The vast majority of economists predict the U.S. will start to rebound later in the year, though they are split over how soon and how fast. Some like Donabedian see a rapid recovery starting in the summer. Others predict a short recession that extends through the fall.
The more optimistic view is based on the assumption that the U.S. approach to containing the coronavirus more closely mirrors that of South Korea or Hong Kong than Italy or Iran.
[...]
“We think we will see a nice bounce back in the third quarter,” Guatieri said.
Still, even relative optimists such as Guatieri say there’s still too much uncertainty to feel confident. He and Wells Fargo’s Bullard say their firms have been changing their forecasts almost daily in the past week as the situation deteriorated. What’s made matters worse is simply not knowing the scope of the problem
“We’re not getting the insight into where we are or where we are going,” Bullard said. “So we’re all just speculating.”
My opinion
Like many of the forecasts above, the articles are very vague about what they expect, and it's hard to see what values are being plugged into these economic models, or whether their prediction is intuition alone.
Conclusion
I have not seen strong evidence that economic forecasters are now predicting doom. However, I have seen some weak evidence that suggests that many are misinformed about the scope of the virus, and its potential future impacts. Some forecasters, like JP Morgan, have clearly done a lot of research. Other firms are barely even using mathematical models of the virus. My own interpretation is that the places I surveyed are probably fairly overoptimistic, though it's really hard to tell without more evidence and concrete numbers.
Replies from: Vaniver, romeostevensit↑ comment by Vaniver · 2020-03-14T00:25:05.554Z · LW(p) · GW(p)
The idea that smart investors don't understand exponential curves is absurd on its face
I don't think this is necessarily absurd or false. Like, this is what Black Swan Farming was about.
I think people in finance are used to exponential curves with doubling times of 20 years, and this doesn't give them much of an edge when it comes to doubling times of 2 days. Like, even in semiconductor manufacturing, the progress of Moore's Law over someone's 40-year career corresponds to about a month of viral growth at that rate.
Startup finance people do work with stuff at roughly the same scale, and correspondingly freaked out much more.
The sheer insanity of such a prediction should give you an idea of how uncertain this whole thing still is.
I don't think this is crazy, once you consider healthcare system failure. What does the world look like if no one receives medical care for any condition besides a COVID infection for the next three months?
↑ comment by romeostevensit · 2020-03-19T00:59:02.460Z · LW(p) · GW(p)
I don't have a strong stance either way but I think there are some interesting points for the other side. Let's say this is on the order of a ww2 number of deaths. Look at the impact of ww2 on the economy. Except with the present situation there's no need to halt international trading, and none of the productive assets get bombed. This still leaves a lot of room on the side of it being worse than many of these sunny projections, but what I want to point at is that it is also really common to drastically underestimate how bad things can look locally and still have trends mostly do alright due to the enormous differences of scale between what it takes for things to look bad and what it takes for things to be bad everywhere.
comment by AlexSchell · 2020-03-11T22:26:45.494Z · LW(p) · GW(p)
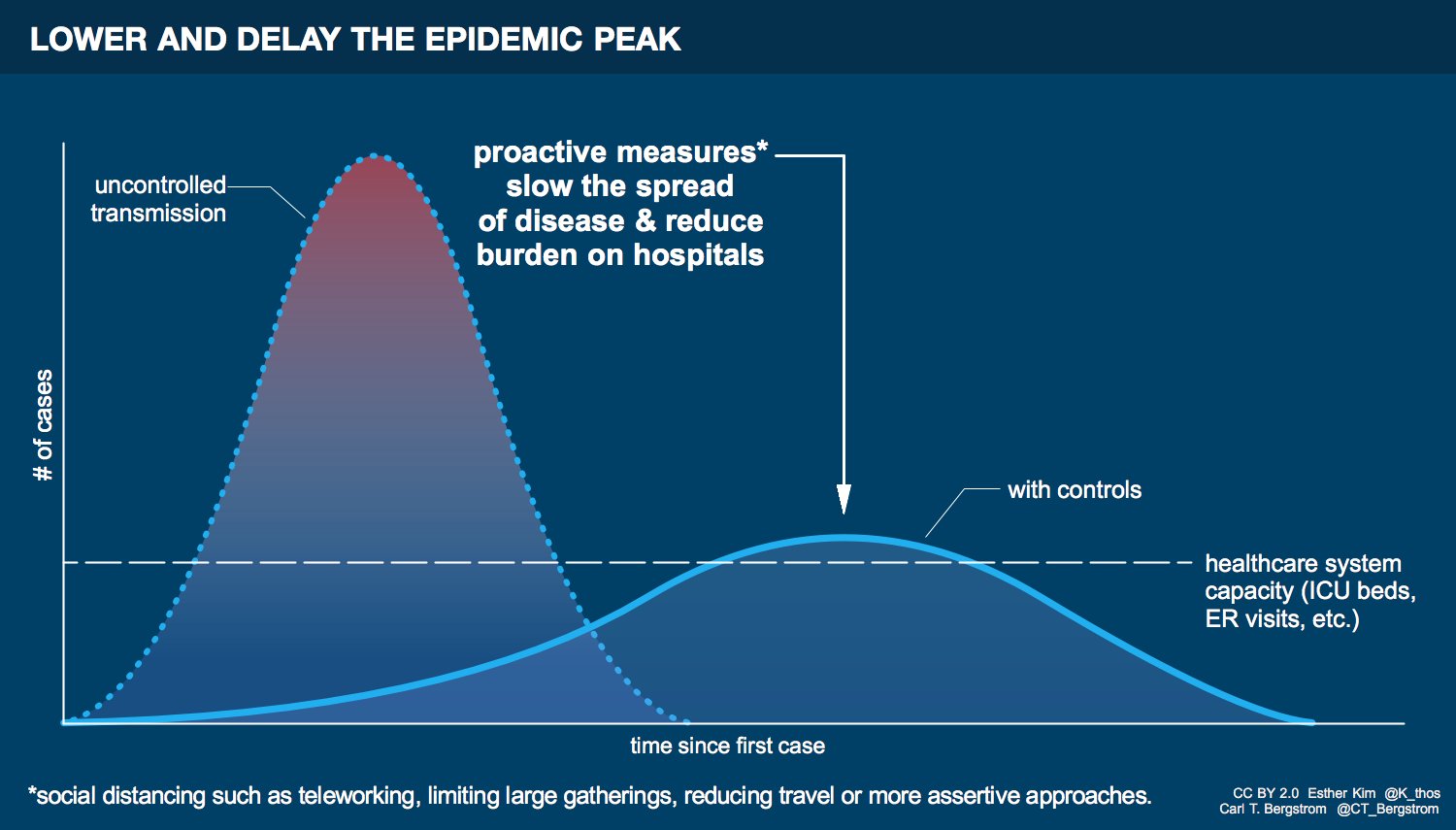
This blog post argues that the now popular idea of "flattening the curve", in the sense that most people get exposed but slowly enough to not overwhelm the health care system, is not feasible. The result is that we'll either achieve containment or at least widespread regional health care system collapse (and maybe Wei Dai's global health care collapse outcome [LW(p) · GW(p)]). I haven't spent much time modeling this yet, but tentatively it looks like flattening the curve requires very precise fine-tuning of R0 to stay on a path very close to 1 for at least several months, which seems impossible to pull off.
It feels to me now that flattening the curve is just a nice graphic without anyone checking the math, but I am confused that many informed-seeming experts are promoting the idea. Anything I'm missing?
ETA: I made an epidemic + hospitalization model (Google Sheets), it sure looks like the usual flatten-the-curve chart is a comforting fiction. Peak hospital bed demand in the uncontrolled epidemic scenario is usually drawn at 2-3x hospital capacity. I'm getting 25x and the chart looks a lot less reassuring. My shakiest assumptions are hospitalization / intensive care rates, any feedback there would be very helpful.
Replies from: paulfchristiano, gwillen, Wei_Dai, Unnamed, Bucky, jmh, jmh, zby↑ comment by paulfchristiano · 2020-03-12T02:36:09.213Z · LW(p) · GW(p)
Disclaimer: I don't know if this is right, I'm reasoning entirely from first principles.
If there is dispersion in R0, then there would likely be some places where the virus survives even if you take draconian measures. If you later relax those draconian measures, it will begin spreading in the larger population again at the same rate as before.
In particular, if the number of cases is currently decreasing overall most places, then soon most of the cases will be in regions or communities where containment was less successful and so the number of cases will stop decreasing.
If it's infeasible to literally stamp it out everywhere (which I've heard), then you basically want to either delay long enough to have a vaccine or have people get sick at the largest rate that the health care system can handle.
Replies from: SDM, AlexSchell, Roko↑ comment by Sammy Martin (SDM) · 2020-03-13T18:40:27.921Z · LW(p) · GW(p)
If it's infeasible to literally stamp it out everywhere (which I've heard), then you basically want to either delay long enough to have a vaccine
South Korea, Singapore, Italy
or have people get sick at the largest rate that the healthcare system can handle.
The UK.
We're running an interesting experiment to see which approach works. One potential benefit is that the world will be able to observe which of the two strategies is viable and switch between them, at least theoretically. Practically, switching from 'suppress/contain' to 'flatten curve' seems a lot more feasible than the alternative of trying to suppress after not taking tough measures, as the UK will have to do if its strategy means cases grow out of control. South Korea could still try to use curve-flattening as a backup plan.
However, for the reason given in the blog post, suppression will be a viable backup even if switching from curve-flattening to suppression is intrinsically harder than the other way round.
The interventions of enforced social distancing and contract tracing are expensive and inevitably entail a curtailment of personal freedom. However, they are achievable by any sufficiently motivated population. An increase in transmission *will* eventually lead to containment measures being ramped up, because every modern population will take draconian measures rather than allowing a health care meltdown. In this sense COVID-19 infections are not and will probably never be a full-fledged pandemic, with unrestricted infection throughout the world. It is unlikely to be allowed to ever get to high numbers again in China for example. It will always instead be a series of local epidemics.
↑ comment by AlexSchell · 2020-03-12T09:12:45.175Z · LW(p) · GW(p)
Still seems to me like you should be able to isolate those problem areas from the rest of the country. Then even if you can't contain the epidemic inside, you spare most of the country (for the moment). But I think we mostly agree. A scenario that seems increasingly likely to me is that governments will intervene in increasingly strict ways until we get very close to true containment (before ~15% of the world is infected), and then will loosen movement restrictions in more-contained areas while playing whack-a-mole with a sequence of localized outbreaks for 1-2 years until a vaccine is ready.
↑ comment by Roko · 2020-03-19T14:39:28.117Z · LW(p) · GW(p)
soon most of the cases will be in regions or communities where containment was less successful and so the number of cases will stop decreasing. If it's infeasible to literally stamp it out everywhere (which I've heard),
Borders, travel restrictions, cancellation of large events, contact tracing and testing will solve this.
Borders are necessary precisely because of this dispersion issue.
↑ comment by gwillen · 2020-03-11T23:39:59.977Z · LW(p) · GW(p)
That's an interesting question that seems like it ought to be able to be checked numerically.
I made an attempt using this simulator of the fairly-naive "SIR" model of disease transmission:
Note that this simulator appears to be someone's class project. However, its behavior seems to track more or less with what I'd expect. But I'd love for someone with more experience to reproduce this relatively simple model and check it.
You can read about the model at https://en.wikipedia.org/wiki/Compartmental_models_in_epidemiology#The_SIR_model .
I have limited confidence that I've understood it correctly, so take this for what it's worth. It looks to me the time step used in this simulator is one day. So the gamma parameter (rate of recovery per unit time) should be (Wikpedia says) 1/D where D is the duration of the disease. (For transmission modeling purposes, this should be the infectious duration, not the duration of symptoms.) I chose gamma=0.7, meaning D ~= 14 days, semi-arbitrarily, based on https://www.medrxiv.org/content/10.1101/2020.03.05.20030502v1 (which says 10 days after start of symptoms) and the general figure of 14-day quarantines.
The beta parameter is the transition rate from "susceptible" to "infected" per person infected per unit time. (That is, betaI is the transition rate overall.) I think therefore R = Dbeta (the total number of new infections per person should equal the duration times the number of infections per unit time), so beta = R/D = R*gamma.
All that being said, given those assumptions, here are what I think the plots look like for various R values. (Note that the names of the parameters given in the URL do not appear to match the names in the UI. I think the URL parameter names are just wrong; the model behaves as I would expect it to. It's a very simple model and I'd love for someone to independently check this.)
R=4.82 (beta=0.34) (upper cited estimate from Wikipedia): http://www.public.asu.edu/~hnesse/classes/sir.html?Alpha=0.344&Beta=0.07&initialS=1000&initialI=100&initialR=0&iters=50
R=3.5 (beta=.25): http://www.public.asu.edu/~hnesse/classes/sir.html?Alpha=0.25&Beta=0.07&initialS=1000&initialI=100&initialR=0&iters=50
R=2.28 (beta=.16) (estimate based on the Diamond Princess data, https://www.ncbi.nlm.nih.gov/pubmed/32097725): http://www.public.asu.edu/~hnesse/classes/sir.html?Alpha=0.16&Beta=0.07&initialS=1000&initialI=100&initialR=0&iters=50
R=2 (beta=.14): http://www.public.asu.edu/~hnesse/classes/sir.html?Alpha=0.14&Beta=0.07&initialS=1000&initialI=100&initialR=0&iters=50
So it looks to me like very substantial curve-flattening ought to be possible, based on this simplified model, at quite realistic R values. Whether it's possible to flatten it enough to prevent health system overload is anybody's guess -- likely not everywhere -- but it looks like there are substantial benefits possible.
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T07:58:44.626Z · LW(p) · GW(p)
Thanks for pointing me in this direction. I think the key worry highlighted in the post is that the health care system gets overwhelmed with even just a few percent of the population being infected. So even if we can bring peak infections down by a factor of 2-4 by slowing transmission, the health care system is still going to be creamed at the peak.
I've now built a discrete-time, Bay Area version of the SIR model (+ hospitalization) in this Google sheet. I assume 20% of infections need hospitalization, of which 20% need intensive care, and use raw bed-to-population ratios (non-COVID utilization vs stretching capacity should roughly cancel out). Hospital bed availability at peak infections is 4% (25x over capacity) in the uncontrolled beta=0.25 scenario and only improves to 10% (10x over capacity) in the "controlled" beta=0.14 scenario. Even if my hospitalization/ICU numbers are too high by a factor of 5 the "controlled" scenario still looks pretty terrible. Any feedback on the model assumptions would be super useful.
Replies from: gwillen, WilliamKiely↑ comment by gwillen · 2020-03-12T08:08:10.734Z · LW(p) · GW(p)
I haven't checked your models quantitatively, but qualitatively I absolutely believe you that the options here are "bad" and "really really bad", and that neither one of them gets us down to where we need to be.
The difference between 4% and 10% could still save a lot of lives; at that level it may be close to 1:1 (every bed freed up is a life saved), since only the most critical cases will be getting beds at that point.
But you're right that this is clearly not adequate, and the graphic showing the flatter curve as peaking under the capacity line is pretty misleading. (There are versions of the graphic which don't, but they appear to have been memetically outcompeted by those that do.)
I think it's still true that "flattening the curve" will save lives, potentially a lot of lives, so even if the graphic might be a bit misleading as to the possibility of flattening it below the critical threshold, I think it's still a reasonable meme to promote.
But really the ultimate goal has to be reducing R below 1, which will arguably flatten the curve, just not quite in the way the meme seems to be trying to get at. I don't want to steer too close to dark side epistemology here, but if the meme gets people to stay inside, cancel their parties, and wash their fucking hands... it's hard for me to be too against it, and I think it's probably true enough?
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T08:58:01.632Z · LW(p) · GW(p)
I don't know how other people react. I took the epidemic fairly seriously but my initial reaction to the meme was one of reassurance/complacency - OK so I can't avoid eventual exposure anymore, but at least things will proceed in a somewhat orderly fashion if we cancel big events, wash hands, stop touching our face, etc. I feel like this is the sort of attitude that contributes to, and allows the public to accept, decisions like the capitulation in Sacramento. The mental image of mitigation is "basically trying to mitigate the risk to those who are most at risk: the elderly and those with chronic underlying conditions". The reality is that we'll be forced to let all the old and sick die in hospital parking lots.
It seems to me fairly likely that the public will ultimately accept the Hubei-style lockdowns that will result in containment, but this meme probably is responsible for delaying that moment by at least a few days :(
Replies from: Raemon↑ comment by Raemon · 2020-03-12T16:18:09.618Z · LW(p) · GW(p)
I saw the meme as mostly targeting people who were currently even more complacent "eh, there's nothing we can do, so fuck it", and getting them to instead go "okay, there's stuff that's actually worth doing."
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T18:01:54.780Z · LW(p) · GW(p)
You're probably right.
↑ comment by WilliamKiely · 2020-03-14T08:19:40.981Z · LW(p) · GW(p)
Hospital bed availability at peak infections is 4% (25x over capacity) in the uncontrolled beta=0.25 scenario and only improves to 10% (10x over capacity) in the "controlled" beta=0.14 scenario.
Alex, I'm looking at your spreadsheet and I don't understand where you got these bold numbers from. It looks like you tweaked your sheet a bit since writing this comment, but still I can't figure out what you are looking at when you say 25x and 10x over capacity. Could you explain?
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-14T08:53:51.665Z · LW(p) · GW(p)
Yeah I got better hospitalization/ICU rates from Bucky and upped beta to 0.3 in uncontrolled scenario to make a point on Twitter. Hospital/ICU bed availability % is graphed in each scenario tab, by overcapacity I mean the inverse of availability. Alternatively take ratio of peak to line in the Charts tab. Looks like ~15x and 5x now for hospital beds.
↑ comment by Wei Dai (Wei_Dai) · 2020-03-12T00:20:02.472Z · LW(p) · GW(p)
That's a really interesting blog post, and it made me update (towards the idea that containment efforts in most countries will keep ramping up until containment actually succeeds). How did you come across it? I've been following Twitter, a couple of FB groups, and Reddit, and it didn't get linked by any of the posts I saw.
It feels to me now that flattening the curve is just a nice graphic without anyone checking the math, but I am confused that many informed-seeming experts are promoting the idea. Anything I’m missing?
I'm wondering this too.
Replies from: AlexSchell, SDM↑ comment by AlexSchell · 2020-03-12T05:45:43.092Z · LW(p) · GW(p)
Don't recall how I ended up seeing it, but it was through this tweet by the author: https://twitter.com/DanielFalush/status/1236918870780198912 (ETA: Razib Khan RT'd him)
↑ comment by Sammy Martin (SDM) · 2020-03-13T21:22:03.408Z · LW(p) · GW(p)
Perhaps the numbers work out better when you include cocooning of populations that disproportionately make use of hospital resources [LW · GW]
↑ comment by Unnamed · 2020-03-12T08:35:35.499Z · LW(p) · GW(p)
I think each little bit of curve flattening makes things a little less bad (since a smaller number of cases are beyond capacity, and a little more time is created to prepare), but the graphs tend to draw the "capacity" line unrealistically high. This graph is more realistic than many since the flattened curve still peaks above the capacity line, but it still paints too rosy a picture.
{kind=link}
↑ comment by Bucky · 2020-03-12T22:11:02.541Z · LW(p) · GW(p)
Nice model.
For hospitalisation / intensive care, the original data from China had 14% "severe" and 5%"critical" cases. These are percentages of diagnosed cases so you would need to modify these with the diagnosis rate.
For the Diamond Princess about 50% of cases were asymptomatic so that is likely an upper limit on diagnosis rate. Ascertainment rates from these papers are highly variable so an actual number here is hard to estimate.
That suggests hospitalisation is probably no more than 10% and intensive care no more than 2.5%. These numbers are a bit lower than your model but not enough to get us out of the woods.
Replies from: SDM, AlexSchell↑ comment by Sammy Martin (SDM) · 2020-03-13T18:46:23.794Z · LW(p) · GW(p)
From the blog post:
If most people who need it do not have access to ventilators, which is inevitable if even a percent of the population are infected at any one time, then it on the order of 4% of infected individuals will die.
I have heard '5-15% [LW(p) · GW(p)]' and '20%' and '12% [LW · GW]' for hospitalization/'no-treatment fatality' rates, with a trend that the newer estimates tend to be lower. The initial figure from China was a blood-curdling 20%, as you said, while a current projection based on evidence from real overwhelmed healthcare systems is a merely very bad 3-5%. This is lower by a larger factor than most of the reductions to the CFR that account for undocumented cases - perhaps indicating there are more undocumented cases than those corrections imply?
Also, of relevance to the UK's strategy (cocooning older people from infection), how does this breakdown by age? This poster has estimated that young, male, no pre-existing condition have 1/4th the risk of hospitalization [LW · GW](assuming a 50/50 chance that the intersection of age-30/no-pre-existing condition has a much lower risk than either alone) - which means if older and vulnerable people can be 'cocooned', the actual rate of hospitalization can be slashed again by a factor of 4 to something bearable, around 1%, if you take 4% as the baseline.
(note that the corrections in this paper for delay to death and underreporting skew the death rates even more strongly towards older patients, with the fatality rate among 20-29 barely changing after adjustment but the fatality rates among 60+ doubling).
{kind=link}
That means you could surf a wave of a few hundred thousand people having the virus at a time and still provide adequate ICU space. With some expansion in capacity, that could be even higher.
↑ comment by AlexSchell · 2020-03-13T06:29:03.936Z · LW(p) · GW(p)
Thanks for digging these up! I updated the model. Still terrible.
↑ comment by jmh · 2020-03-12T21:06:15.199Z · LW(p) · GW(p)
I'm wondering why you are also coming up with a LOT more hospitalization than even cases reported in China.
In early April, if I'm readying this right, you are expecting the Bay area to need over 80,000 hospital beds for COVID-19 for the uncontrolled case (I assume that is merely a comparison scenario) and then after 3 months, say starting July, in the controlled scenario about 81,000 hospital beds will be needed. Then things keep going up.
That seems like something is missing there. Why would the Bay area really expect to see such drastically higher impact than China as a whole? Using your 20%, 20% assumption and saying China is at 85,000 now, the total demand for hospital beds would have been 20,400 over the entire December - March time period.
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T22:22:30.179Z · LW(p) · GW(p)
China locked down Wuhan at ~500 confirmed cases and many other Hubei cities the next day, which immediately lowered transmission (see Chart 7 here) to R0 below 1. This is very far from the uncontrolled scenario and still overloaded the health care system. This is much of the point of the post I linked -- the degree of hospital overload in an uncontrolled scenario is so high that even huge reductions in transmission don't realistically avoid overload if R0 stays above 1.
Replies from: jmh↑ comment by jmh · 2020-03-13T14:10:09.966Z · LW(p) · GW(p)
I do get that point, and do think it is one that is well made. At the same time, I find the numbers produced a bit on the high side. Clearly the 20,400 number being within existing capacity for the Bay area completely ignores current patients unrelated to COVID-19. But perhaps under a regime of social distancing, containment and isolation of both known cases and by the more concerned both the speed of growth and the total number your model is producing would be much closer to manageable.
↑ comment by jmh · 2020-03-12T20:43:10.108Z · LW(p) · GW(p)
I think it might also be worth considering hospital beds -- to some extent -- is not a fixed quantity to can expand as demand increases. Consider using hotels or other (these days rather vacant) building/structures. That's basically what China has done here (and in other cases with their "legos" 10 day to build hospitals -- rejected the concept of what a hospital is and how fixed the supply is.
Just as an assumption check, was your hospital bed/ICU bed value an average for, say the USA, or some other country level metric or an average of the local hospital to service area metric?
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T22:27:17.280Z · LW(p) · GW(p)
I used overall US numbers. I didn't consider capacity expansion but also didn't take out already-occupied beds, as I think both are roughly on the order of 2-5x in opposite directions. The only Bay Area-specific numbers are population and day 0 infected (I assumed ~10x confirmed cases).
↑ comment by zby · 2020-03-12T16:34:24.406Z · LW(p) · GW(p)
It worked in 1918: https://qz.com/1816060/a-chart-of-the-1918-spanish-flu-shows-why-social-distancing-works/
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T18:00:26.928Z · LW(p) · GW(p)
I should have made it clearer I don't deny we can literally flatten the curve, but rather the idea that
most people get exposed but slowly enough to not overwhelm the health care system.
Unclear to me how well St Louis did on the health care system front. Also, the pairing of Philadelphia and St Louis is a bit convenient if you consider the raw scatterplot (panel C bottom left - ETA Philadelphia is the dot closest to Pittsburgh per this table).
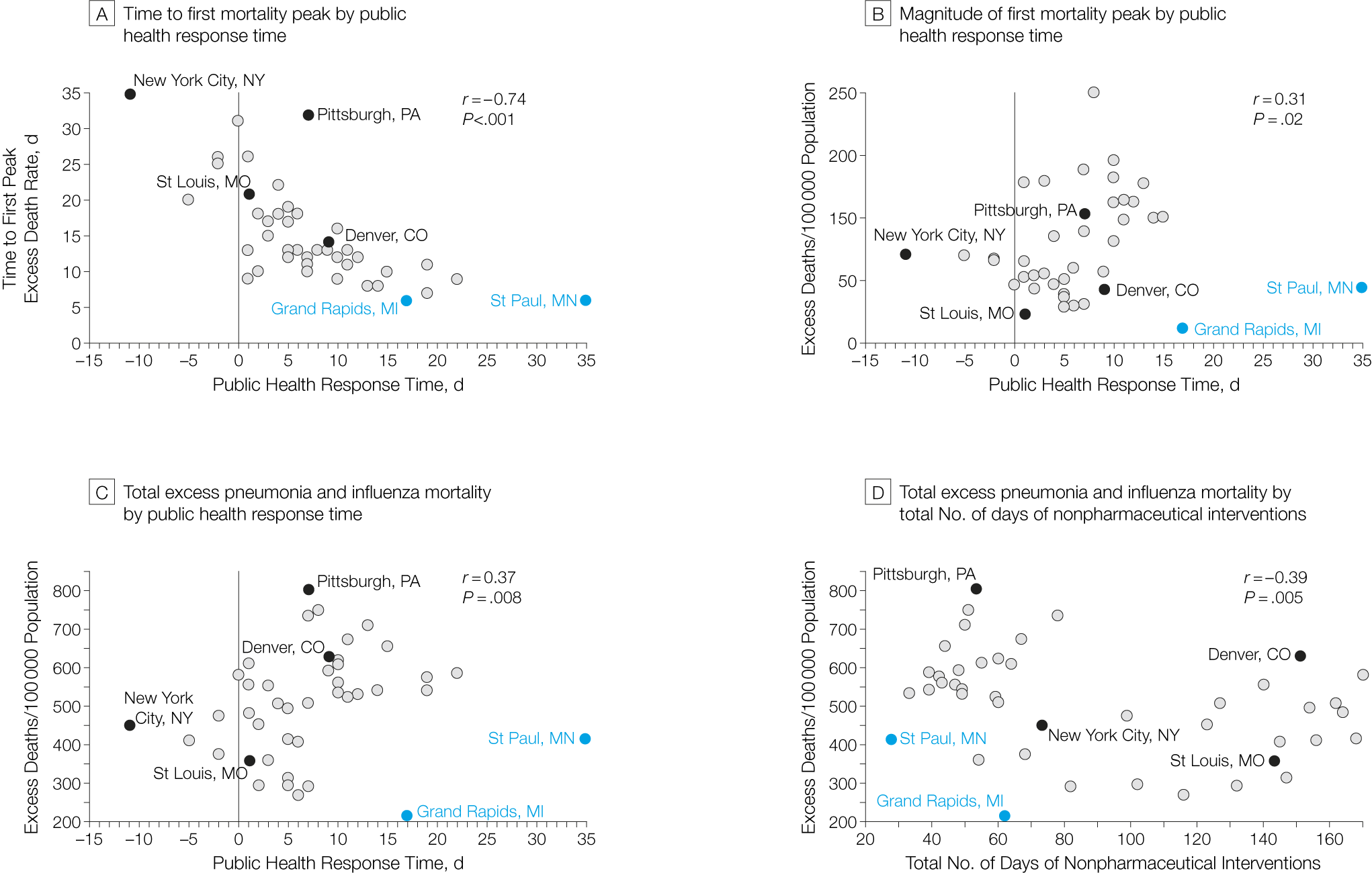{kind=link}
{kind=link}
comment by Pablo (Pablo_Stafforini) · 2020-03-09T01:22:16.306Z · LW(p) · GW(p)
I think it would be valuable to compile a list of estimates of basic epidemiological parameters of the coronavirus, such as incubation rate, doubling times, probability of symptomatic infections, delay from disease onset to death, probability of death among symptomatics, and so on. I find that my inability to model various scenarios accurately is often due to uncertainty about one or more of these parameters (uncertainty relative to what I suspect current expert knowledge to be, which is of course also uncertain to a considerable degree).
Replies from: Bucky, kdbscott, elityre, habryka4, romeostevensit, rocurley↑ comment by Bucky · 2020-03-10T16:45:41.630Z · LW(p) · GW(p)
For current expert knowledge, this list of values from lots of different papers might be helpful.
Replies from: Pablo_Stafforini↑ comment by Pablo (Pablo_Stafforini) · 2020-03-11T14:47:10.620Z · LW(p) · GW(p)
Wonderful, thank you so much.
↑ comment by kdbscott · 2020-03-15T07:27:51.956Z · LW(p) · GW(p)
Did you end up finding one besides the MIDAS network, or develop your own? I'm assembling a parameter doc for inputs to a rough model that accounts for ventilator & hospital bed capacity, since it seems like we're lacking that.
- I encourage folks to add parameters w/ citations to the doc, I'll be active on it for the next few days.
- If anyone knows of models that incorporate actual healthcare capacity, please share!
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-15T18:34:06.797Z · LW(p) · GW(p)
Thanks for putting this list together.
I stopped looking after Bucky supplied the link to the MIDAS network list, since it seemed so comprehensive.
For models that incorporate actual healthcare capacity, see this thread [LW(p) · GW(p)]. One limitation of the models I've seen is that they fail to account for growth in such capacity. China responded to the realization that they didn't have enough hospitals by quickly building more hospitals. Maybe Western countries are less competent than China and it will take them longer to build the needed capacity. But it seems implausible that they will be so incompetent that capacity-building efforts will not make a significant difference.
↑ comment by Eli Tyre (elityre) · 2020-03-10T07:09:09.857Z · LW(p) · GW(p)
Having a list of of values of interest, with estimates and citations for each, would be great.
But in addition, I gotta say, this seems like just about a perfect use-case for prediction markets: we have a bunch of individual, well operationalized scalars, for which accurate estimates that incorporate all of the existing information are of high value.
Is anyone in a position to set up, or to subsidize, a market on these values?
↑ comment by habryka (habryka4) · 2020-03-09T02:30:38.773Z · LW(p) · GW(p)
I second this.
↑ comment by romeostevensit · 2020-03-19T01:05:27.794Z · LW(p) · GW(p)
And to start compiling a list of common problems with the parameter estimates being used. Eg I am seeing some models extrapolate naively from the fact that most cases are coming from the least controlled places with the widest uncertainty bars.
↑ comment by rocurley · 2020-03-09T17:08:01.909Z · LW(p) · GW(p)
I'm also very interested in this. Here are some numbers I've been using:
- Ratio of confirmed to unconfirmed cases (USA):
34 (50%), or 5 (5%) to 94 (95%)
This is based on https://twitter.com/trvrb/status/1234589598652784642 , which estimated the true number of coronavirus cases in Seattle (as of 2020-03-01). I divided that by the number of confirmed cases in Seattle at that time.
- Doubling time (USA):
4 ish (which I'm treating as 2 (5%) to 7 (95%). https://en.wikipedia.org/wiki/Template:2019–20_coronavirus_outbreak_data/WHO_situation_reports is how I'm getting 4ish. There are papers that estimate higher: https://www.nejm.org/doi/full/10.1056/NEJMoa2001316 gives 7, for example, but that appears to be in Wuhan post-containment.
Replies from: jmh↑ comment by jmh · 2020-03-09T17:39:07.962Z · LW(p) · GW(p)
South China Morning Post had a story line a day or so back where Chinese experts were suggesting a 10 fold increase every 19 days. Interestingly the rate seems to be about double that if you look at the last 19 days.
I did not look past the totals but suspect that is highly dominated by South Korea (seems to be slowing), Italy and Iran (these two do not seem to be slowing).
Might also be interesting to put a latitude metric in as well -- while I have a "sense" that more equatorial areas have a lower incident (and may be spread rate) I've not seen that data plotted anywhere.
comment by Spiracular · 2020-03-18T01:09:30.702Z · LW(p) · GW(p)
Paper on some of nCOV's mutations
Incidentally, also strong evidence against it being a lab-strain. It's a wild strain.
Closest related viruses: bats and Malayan pangolins
Mutation Descriptions
Polybasic Cleavage Sites (PCS): They seem to have something to do with increased rates of cell-cell fusion (increased rate of virus-induced XL multi-nucleated cells). Mutations generating PCS have been seen in Influenza strains to increase their pathogenicity, and they had similar effects in a few other viruses. So it's not exactly increasing virus-cell fusion, it's actually... increasing the rate at which infected cells glom into nearby cells. Fused cells are called syncytia.
O-linked glycans : Are theorized (with uncertainty) to help the virions masquerade as mucin, so hiding from the immune system. (Mutation unlikely to evolve in a lab on a petri dish)
Arguments strongly in favor of it being a wild strain
- It's not that similar to one of the known lab-strains, so it probably was wild
- The "polybasic cleavage site" and "O-linked glycans" mutations would have required a very human-like ACE-protein binding site, so basically only human or ferret cells
- O-linked glycans are usually evolved as an immune defense, which isn't something cell cultures do.
(Just following the recommendation to move this out of shortform so it can be tagged later.)
Replies from: Spiracular, Spiracular, ChristianKl, Spiracular↑ comment by Spiracular · 2020-09-15T19:07:45.159Z · LW(p) · GW(p)
Chinese virology researcher released something claiming it SARS-2 might even be genetically-manipulated after all? ZC45 and/or ZXC21 backbone. Claims that the RaTG13 genome was a concocted cover-up. After assessing, I'm not really convinced of the GMO claims, but the RaTG13 story seems to have something weird going on.
https://zenodo.org/record/4028830#.X2EJo5NKj0v
See here [LW(p) · GW(p)] for my further thoughts on this.
EDIT: After assessing, I'm not finding the GMO claims convincing. The RaTG13 story does seem to have something weird going on, and there's several people and papers that note weird inconsistencies (See the further thoughts, I don't have a simple explanation.).
↑ comment by Spiracular · 2020-04-02T09:52:53.910Z · LW(p) · GW(p)
Additional little bit that reminded me of that cell-cell fusion trait... another paper described the SARS-CoV-2 autopsy results, and included this:
Multinucleated syncytial cells with atypical enlarged pneumocytes showed viral cytopathic-like changes, without obvious intranuclear or intracytoplasmic viral inclusions.
Translation: The paper-thin, high-surface-area (for gas exchange) cells wrapping your lung balloons (the pneumocytes in your alveoli) fuse together with each other into an ineffectual, clumpy mess with a way lower surface-area-to-volume ratio. These are fragile cells to begin with; they don't even replicate themselves (other cells have to replace them when they break). They don't seem to be producing virus themselves, but they do seem to be getting badly screwed up by things the virus is doing.
↑ comment by ChristianKl · 2020-04-17T19:50:06.680Z · LW(p) · GW(p)
Incidentally, also strong evidence against it being a lab-strain.
What exactly does "lab-strain" mean here? Does it means a strain with a already published sequence?
Replies from: Spiracular↑ comment by Spiracular · 2020-04-18T20:47:40.977Z · LW(p) · GW(p)
More specifically:
- It was not genetically modified for use as a bioweapon
- The mutations don't resemble other well-known and well-characterized pathogenicity mutations too closely, in sequence or location
- It probably wasn't cultured as cell-culture in a lab-setting for an extended period
- The virus was not notable to science prior to this event
Or in other words, it doesn't look planned. Its most recent mutations look much more like a "natural variation let it jump species" sort of situation.
This doesn't address situations like, for example, "dead bats with a wild-type virus being left near a bunch of ferrets or pangolins," or something to that effect.
(ETA: Or... accidental release like this [LW(p) · GW(p)] is still possible.)
↑ comment by Spiracular · 2020-05-01T02:07:55.377Z · LW(p) · GW(p)
Despite the virus being characterized in pangolins, after looking into this, I now think it is basically incorrect to think of this as primarily a "pangolin virus." The pangolins were a dying canary in a coal mine, and probably caught it from something else that serves as the real reservoir species for this nCOV precursor*.
See: further explanation here [LW(p) · GW(p)]
comment by Slava Matyukhin (berekuk) · 2020-03-10T22:32:36.821Z · LW(p) · GW(p)
Two facts:
- HCoV-OC43 (one of human coronaviruses causing common cold) can generate cross-reactive antibodies against SARS.
- Immunity to HCoV-OC43 appears to wane appreciably within one year.
Here's the paper which mentions both of these facts. (The actual paper is not important, I expect these facts to be well-known to coronavirus researchers, if the paper itself is not terribly mistaken and if I haven't misread anything.)
Even if cross-immunity is mild, won't it make sense to intentionally infect people with HCoV-OC43? Downside seems quite small compared to the number of deaths, and intuitively it seems that "mild cross-immunity" = "less severe SARS-CoV-2 cases", which is extremely valuable.
I notice I'm confused, since these facts should be well-known to pretty much everyone who's working on the vaccine. What's the explanation for why it's not a good idea?
Possible explanations, but I'm probably missing something:
- Vaccines which cause the actual illness are considered unethical. (Probably not? I don't expect humanity to be that stupid.)
- Mass-producing HCoV-OC43 virus is too hard for some reason. (Possible? I don't know much about vaccine production, and I'm clueless about whether it's even possible to mass-produce and store a "live" virus; but this seems solvable through organized infection parties, etc.)
- Researchers or medical organizations don't want to rely on expected utility. Related hypothesis: time and productivity wasted by infecting many people with HCoV-OC43 is too valuable, and infecting everyone with HCoV-OC43 at the same time would hurt economy too much. (I don't believe this, but I haven't really tried to estimate this. If the alternative would be "wait for the real vaccine which is just around the corner", then yes, let's wait, but if the alternative is waiting for 12-18 months, then it doesn't feel right.)
- Maybe I don't understand what "mild immunity" means and it's not that valuable of a perk to intentionally cause it? (But the same paper I quoted talks about HCoV-OC43 importance for predicting future SARS-CoV-2 outbreaks.)
- Maybe being infected with HCoV-OC43 is too risky because getting two viruses at the same time is dangerous? Or because it would confuse the situation and complicate diagnoses of the real SARS-CoV-2? (Maybe... If everyone is sick with common cold then it would help SARS-CoV-2 to spread since everyone would be sneezing and coughing. But it also seems like a question of good timing and at least worth considering.)
So, what am I missing here?
Replies from: pktechgirl, berekuk, Spiracular, gwillen↑ comment by Elizabeth (pktechgirl) · 2020-03-11T01:05:20.679Z · LW(p) · GW(p)
There's speculation that having acquired immunity to similar viruses leads to worse outcomes with COVID-19, and that's why children don't have many symptoms. This is still highly speculative, I won't be surprised if it turns out to be something totally different, but it would make me nervous about this plan.
↑ comment by Slava Matyukhin (berekuk) · 2020-03-11T01:10:01.421Z · LW(p) · GW(p)
Okay, SARS-CoV-2 is pretty different from SARS-2003 ("~76% amino acid identity in the spike protein"), this might be the reason it won't work. OTOH, I don't know how different HCoV-OC43 is from both SARS strains.
↑ comment by Spiracular · 2020-03-15T20:58:41.857Z · LW(p) · GW(p)
Similar to the thing Elizabeth mentioned, I'm concerned about the possibility of antibody-dependent enhancement wherein an imperfect antibody match actually worsens the course of the infection.
I've tried to look into this. My results weren't conclusive, but I think it's a very real possibility for this virus, and fairly likely to slow vaccine development due to the added testing it neccessitates.
↑ comment by gwillen · 2020-03-11T00:51:13.894Z · LW(p) · GW(p)
I would also like to know the answer to this.
One thing I'm not sure about: how hard is it to get your hands on HCoV-OC43? With high confidence and in quantities suitable for pretty much guaranteeing to give someone a cold / some immunity? (Do excessive quantities lead to a more severe cold?)
This does really seem like something someone should be working on. Probably someone is, somewhere...
EDIT: Here is one paper on the consequences of HCoV-OC43 infection:
https://www.ncbi.nlm.nih.gov/pubmed/23337903
Among other things: "Recent studies have suggested [that human coronaviruses] can cause severe lower respiratory tract illnesses in children." and "In our population, HCoV-OC43 infections generally caused upper respiratory tract infection, but can be associated with lower respiratory tract infection especially in those coinfected with other respiratory viruses."
So safety might be in question.
EDIT 2: Scihub link: https://sci-hub.tw/10.1097/INF.0b013e3182812787
EDIT 3: I would really love for someone who knows things to take a look at this paper actually, and help interpret it. It is only studying children, and notes that "HCoV-OC43 infections tend to occur before 2 years of age" (does that mean adults can't get it? or they aren't exposed to it much? Does exposing them to it generate a useful immune response?), and also that, among the children selected for the study, children with HCoV-OC43 had better outcomes than controls (but I have no idea how to normalize this for statistical issues; the subjects were children who tested positive for HCoV-OC43, whereas the controls were children who were tested for respiratory viruses but were negative for HCoV-OC43.)
comment by Eli Tyre (elityre) · 2020-03-14T18:16:53.311Z · LW(p) · GW(p)
This paper is well worth a read, according to me. Given that we have all kinds of problems doing testing for COVID-19 in the US, the authors do an analysis of the ratio of people seeking medical help for flu-like symptoms, but testing negative for the flu, to people testing positive (compared to previous flu seasons). The idea being that if COVID-19 is spreading, we should be seeing increases in flu symptoms relative to flu diagnoses.
However, I'm confused about Arizona. (See figure 4 in the paper). It looks like its score on this axis has been 2 to 3 standard deviations from the mean for the decade since November.
What's going on?
Hypotheses:
- The Flu season in Arizona was so bad this year that the number of people who came in with flu symptoms skyrocketed, relative to other kinds of ailments, and even though most of those people did test positive for the flu, the wILI term swamped the (1 − proportion of tests positive for influenza), for an overall much higher than usual ILI-.
- Is that mathematically plausible?
- There was some other flu-like non-flu that was spreading in Arizona since November.
- The flu diagnosis process spontaneously failed this season, producing orders of magnitude more false negatives, in Arizona, but not in any other state.
- COVID-19 has been spreading in Arizona since November, but somehow there are only 9 serious cases.
- COVID-19 has been spreading in Arizona since November, but testing is so ineffective, that there are hundreds of people with severe phenomena-like symptoms, who have not been recognized as COVID-19 cases, somehow.
What's going on here?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2020-03-15T18:05:23.745Z · LW(p) · GW(p)
Based on figure 4, this would predict that the midwest would have a worse epidemic than the pacific NW right now, and twitter reports from hospitals don't seem to bear that out.
comment by Elizabeth (pktechgirl) · 2020-03-10T20:23:14.174Z · LW(p) · GW(p)
Why are we prioritizing testing the sickest people? AFAIK diagnosis doesn't change what care is given, so it's irrelevant to them. Testing people who might be sick and take high impact action based on the results (e.g. medic deciding whether to go to work) seems higher impact.
Possible explanations: sickest people get the most positives and that's important for contact tracing, I am wrong about how it affects care (in particular it might affect if you get an isolation room or no)
Replies from: gwillen, syllogism, Original_Seeing↑ comment by gwillen · 2020-03-10T20:47:35.387Z · LW(p) · GW(p)
My assumption has been that the primary purpose of testing is for contact tracing. I would suspect that probably don't have enough tests at this point to usefully test everybody who is ill and yet still planning to go to work, even just people with healthcare jobs -- I'm assuming that someone who is ill, but still thinking about going to work at their healthcare job, is probably not very sick, in which case most of those tests would end up negatives, on people who just have colds/flu.
↑ comment by syllogism · 2020-03-14T22:08:05.754Z · LW(p) · GW(p)
Most tests you carry out on anyone else will be negative, so even if you think there's an 80-90% chance the patient is COVID-19 positive, you still get more information from running those tests than the lower symptomatic people.
Also, it does change all sorts of decisions. It probably changes what precautions the healthcare workers need to take, and it lets you tell the person's family to self-isolate. Otherwise the husband is in critical condition, and the wife might be a week behind, so she's in the waiting room making everyone sick.
Replies from: gwillen↑ comment by gwillen · 2020-03-16T00:38:38.044Z · LW(p) · GW(p)
Hm, can you say more about information? I believe you should get the most direct information (in the information-theoretic sense) out of running tests where the outcome is most in doubt (i.e. where your prior is approximately 50%, although I think this might budge a bit depending on the FP/FN rates of the test if they are different.) You also get information about their contacts -- if their contacts have a lower-than-50% base rate of exposure, then it seems like you get more of that "secondary information" from a positive than from a negative. (I'm not too confident about that, but certainly at worst it's equal, right?)
↑ comment by Original_Seeing · 2020-03-12T18:15:44.569Z · LW(p) · GW(p)
An accurate count of how many people are infected may be a highest priority. Since the virus has exponential growth, the difference between a known count of 10 infected vs 100 infected is massive in terms of policy decisions. Undercounting is extremely dangerous to the entire population.
This could change once the number of infected patients gets very high, but we may not have seen numbers high enough to justify that anywhere outside of China yet.
comment by gwillen · 2020-03-10T20:50:01.584Z · LW(p) · GW(p)
Several counties in California are now advising people not to bother self-quarantining at home after COVID-19 exposure unless they get symptoms. This seems wildly irresponsible to me. I understand not wanting to use valuable health system resources on people who are unlikely to have the virus, but home self-quarantine does not cost the health system anything now, and it is likely to save the health system a lot of cases later. Right?
https://www.sacbee.com/news/local/health-and-medicine/article241047391.html
This seems in particular very much at odds with Italy's striking decision to lock down the entire country, including whole regions with no known exposures.
Any thoughts?
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2020-03-10T21:04:30.761Z · LW(p) · GW(p)
Reading between the lines, it sounds like they're no longer contact tracing.
“Once you get a certain number of cases, it’s hard to continue to contact-trace back the way you tried originally,” Beilenson said, “so we move to mitigation, which is basically trying to mitigate the risk to those who are most at risk: the elderly and those with chronic underlying conditions.”
I would interpret this to mean they're not tracking down people to recommend that they, specifically, self-isolate, but it's not a blanket recommendation not to self-isolate. They also don't seem to recommending that, but it's not clear they ever did.
Replies from: gwillen↑ comment by gwillen · 2020-03-10T21:47:57.990Z · LW(p) · GW(p)
I think that would have been a very reasonable thing, but no, it is a blanket recommendation that self-quarantine for known exposure is not required (at least for Sacramento County):
"With the shift from containment to mitigation, it is no longer necessary for someone who has been in contact with someone with COVID-19 to quarantine for 14 days. This applies to the general public, as well as health care workers and first responders. However, if they develop respiratory symptoms, they should stay home in order to protect those who are well. "
comment by gwillen · 2020-03-11T02:04:30.238Z · LW(p) · GW(p)
What are the issues involved in receiving delivery food during this pandemic?
Can one safely receive and eat delivery food as follows: Avoid contact with the deliveryperson (have them leave it outside), carefully dispose of the packaging in the same way you would for a package delivery, then take the delivered food and reheat it in the oven for a time/cooking temp that will kill the virus?
The respiratory viruses as a family do not appear very resistant to heat (as compared to e.g. some of the foodborne illnesses.) From https://www.quora.com/At-what-temperature-does-the-cold-virus-die/answer/Thomas-Basterfield (I didn't check the citations yet), it seems like 70C for 25 minutes will kill most respiratory viruses thoroughly. This is such a low temperature that I wonder if hot food is inherently inhospitable to them even without the reheating step. My oven dial doesn't even go that low. (Getting the center of the food to this temperature could be challenging without using a higher oven temperature, but you really only need to do the surface; the center has already been cooked, and any relevant contamination will be on the surface from post-cooking handling.)
(There is also a mention of autoclaves, which apparently require <300F and <20 minutes at 15 PSI over atmospheric to sterilize surgical instruments. (Eyeballed numbers, do not trust.) In fact, I was able to find a published paper which concludes that a pressure cooker can be used in place of an autoclave with good results, https://www.ncbi.nlm.nih.gov/pubmed/12267939. So a pressure cooker (e.g. an instant pot) seems like another route to ensure delivery food is heated to a temperature that will kill viruses, although it's probably overkill and is likely to damage the texture of some foods, but is maybe a better option for foods that would dry out objectionably in the oven.)
(It also seems very likely to me that a microwave could achieve sufficient conditions for this, although I think it would be harder to be confident about it without at least having a meat thermometer.)
Does this seem like a reasonable approach?
[One thing I still have to figure out: I have been receiving "ready-to-heat" meals from https://www.freshly.com/. They are precooked but refrigerated, and require reheating. I'm not sure what my risk here is, and how much I can reduce it by just heating them longer in the microwave than the instructions call for.]
Replies from: steve2152, Raemon, Raemon↑ comment by Steven Byrnes (steve2152) · 2020-03-25T00:12:58.455Z · LW(p) · GW(p)
I like the discussion in Food Safety and Coronavirus: A Comprehensive Guide. Note that the author has a conflict of interest, but I don't think he let it affect the article.
Replies from: gwillencomment by Roko · 2020-03-18T19:51:52.046Z · LW(p) · GW(p)
An review of Ferguson et al's paper by Nassim Taleb has come out: https://necsi.edu/review-of-ferguson-et-al-impact-of-non-pharmaceutical-interventions
I think this document contains the essential strategy for quickly bringing covid-19 under control. I'll call it "Containment and Eradication":
1. Close national borders
2. Reduce R0 below 1 using a thorough lock-down, social distancing, testing, contact tracing and hygiene
3. Once the outbreak is quite small and testing capacity is decent, aim to drive the number of infected individuals as close to 0 as possible
4. Test aggressively and wait a couple of weeks
5. Gradually return people to mostly-normal life, but with large gatherings cancelled for the foreseeable future due to the possibility of super-spreader events, and international travel mostly cancelled.
6. Keep borders fully closed to until we have a vaccine, or at least impose long quarantine periods on travelers.
Approaches to covid-19 that involve getting a large number of people infected to build herd immunity and minimize the damage along the way are far inferior to this. The Ferguson et al analysis showed us just how messy that would get, but I think it was probably an underestimate of the expected disutility of these "mitigation" approaches, as its estimates of the infection fertility rates didn't take into account the effect of health systems being overwhelmed. Furthermore, attempts to "flatten the curve" impose both economic and human costs for an extended period.
This is the most encouraging thing I have read about covid-19 in a long time. I believe that "Containment and Eradication" is the way forward and that this should be signal boosted.
comment by habryka (habryka4) · 2020-03-16T22:24:37.024Z · LW(p) · GW(p)
As part of the LessWrong Coronavirus Link Database, I am publishing a daily update post with all the new links we are adding each day that we ranked a 3 or above in our importance rankings. Here are all the links we added over the weekend.
Guides/FAQs/Intros
Coronavirus: Why you must act now (medium post)
Summary and call to action, one of the best summaries I've found, focuses more on policy-interventions than on individual actions, but is still good at giving you an overview
UpToDate: Coronavirus Overview
UpToDate very frequently has the best overviews over many crucial medical topics. Geared towards a more professional medical audience.
Letter to loved ones asking to take CV seriously
Well written, compassionate explanation of why this is worse than what we've seen before and need to take this seriously. A few pointers on where to get started
Early February 80,000 hours episode on Coronavirus (1h 18min)
Long episode on coronavirus. Includes all the basic information, and discussion of big-picture implications
Spread & Prevention
Masks help prevent infection in schoolchildren:
In a group of 10,524 Japanese schoolchildren, masks and vaccination decreased the chance of catching influenza, gargling and handwashing increased the chance
Metareview: facemasks at mass gatherings
A collection of 25 studies with 12710 participants was examined. Out of 13 studies on respiratory illness, 4 showed statistically significant effectiveness, 1 showed statistically significant ineffectiveness, the rest produced no statistically significant results
“Flattening the Curve” is a deadly delusion
At current medical capacity, we'd need to flatten the curve for 10 years in order to get everyone full treatment
Summary of papers arguing that many/most infections spread from people before they show symptoms [LW · GW]
A readable summary of some papers about how quickly people transmit the disease and how quickly the symptoms show. Argues that perhaps the majority of people transmit it before they show symptoms.
Timothy Gowers: Herd immunity is very costly, and we can't get all the things we ant
Twitter thread on costs of UK's herd immunity strategy, argues that we have to give up at least one of: (1) herd immunity (2) non-overwhelmed hospitals (3) get life back to normal before next winter
Paper: derives CV prevalence estimates from data on unexplained flu-like symptoms
The relative prevalence of patients influenza like illnesses that test negative for influenza has been high for the past several weeks, but not extraordinarily so (< 3 standard deviations)
Rob Wiblin: Model update suggests we are dealing with unmitigated exponential growth
Rob Wiblin updated his spreadsheet model with new data, which suggests that we are basically dealing with unmitigated exponential growth, without any significant slowdown
Progression/Outcome
Twitter: CV kills via cardiac failure, not pulmonary
Aapparently the ARDS is not too severe, and they can manage people through that part of it. Instead, after several days, the virus suddenly attacks the heart, causing it to precipitously fail. The myocarditis phase is savage and kills people within a day or two
Tries to produce more accurate death-rate estimates for China, South Korea, and Italy, based on interpretation of existing data
Seattle ICU Dr describes CV progression
The Chinese data on 80% mildly ill, 14% hospital-ill, 6-8% critically ill are generally on the mark, elderly patients going to "comfort care", detailed description of clinical presentation, remdesivir is scarce
Doctor reports 20-30% reduction in lung capacity in 1/4 of patients
News report on a doctor saying that 2 or 3 out of 12 patients have seen a 20-30% reduction in lung-capacity and "They gasp if they walk a bit more quickly"
Medical System
Twitter: Seattle approaching Lombardy levels
Seattle has ventilators but is out of ICU beds. Due to a lack of machines, Seattle is restricting ECMO machines to people <40 yo and < 25 BMI. Most people are dying of heart, not lung, issues
Twitter: Seattle ICU Dr describes conditions in Seattle hospital
Entire ICU taken up by CV patients, CDC is weakening quarantine on medics, they are out of masks in part because people are stealing from them
Jess Riedel's Fermi Estimate that not containing coronavirus will overwhelm UK medical system
Jess Riedel's Fermi Estimate that not containing the coronavirus will overwhelm the UK medical system
Dashboards
Very comprehensive dashboard with dozens of graphs. Currently the best resource I know for tracking both national and global spread.
Aggregators
Surprisingly high-quality of articles on the Medium coronavirus page.
Aggregators
Effective Altruism Facebook group on Coronavirus discussion
Facebook group with lots of members of the EA community discussing various considerations and plans
Other
[TEMPLATE] Coronavirus Household Isolation Coordination v1.2
Spreadsheet for keeping people in your social network up-to-date with each other's health and social distancing status
Why now is a time of great opportunity for helping the world [LW · GW]
Detailing what opportunities are available (contact tracing, building entilators, remote work tech, etc) and framing why to take action and how.
Link to Full Database
comment by jefftk (jkaufman) · 2020-03-09T15:40:14.107Z · LW(p) · GW(p)
How useful is it to heat your house to 75F+? To heavily humidify your house?
Replies from: jp, ady-jade-beacham↑ comment by Ŀady Jade Beacham (ady-jade-beacham) · 2020-03-09T19:09:26.640Z · LW(p) · GW(p)
Do you expect transmission to occur within your house? From a guest? Or at a grocery store or outside contact? Seems like it would only help in the in-house case. I expect this to be pretty far down the list of useful interventions
Replies from: gwillencomment by Jayson_Virissimo · 2020-03-09T03:35:45.404Z · LW(p) · GW(p)
I’ve been keeping notes on corona virus risk reduction tactics and turned some of them into a webpage to share with my family and friends. The idea to to make them as quickly actionable/understandable as possible. This is the pretty version, but you can contribute here.
I'm very interested in critical feedback, including if any of these tactics are likely to be harmful/ineffective or if I'm missing anything high-value/low-cost.
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-09T19:25:16.792Z · LW(p) · GW(p)
I consider my copper wrapped stick [LW · GW]to be a high-value/low-cost option. It allows me to open door handles/light switches without having to touch them with my hands.
comment by PeterMcCluskey · 2020-03-30T02:11:43.187Z · LW(p) · GW(p)
A new paper: Correlation between universal BCG vaccination policy and reduced morbidity and mortality for COVID-19: an epidemiological study says that vaccination for tuberculosis has a potentially large effect on COVID-19 problems. This explains some of the strange differences between countries. That's bad news for the U.S. (which hasn't required the vaccine), good news for some countries.
Replies from: gwillen↑ comment by gwillen · 2020-03-30T07:02:16.491Z · LW(p) · GW(p)
That's extremely interesting. I would love to see someone in our community who I trust to be good at statistics redo the analysis, since all the data is public.
Apparently there are already multiple trials underway, though: https://www.sciencemag.org/news/2020/03/can-century-old-tb-vaccine-steel-immune-system-against-new-coronavirus . The Science article came out before the paper, so I wonder where the idea struck first.
Apparently the broader pro-immune effects of the BCG vaccine for tuberculosis have been known or suspected for a long time; see e.g https://www.ncbi.nlm.nih.gov/pubmed/31055165 "Non-specific effects of BCG vaccine on viral infections", http://sci-hub.tw/10.1016/j.cmi.2019.04.020, which is a fucking wild read and I highly recommend reading the whole paper.
Replies from: zby↑ comment by zby · 2020-03-30T07:41:26.544Z · LW(p) · GW(p)
It is also a hope in type 1 diabetes: https://www.google.com/search?q=bcg+diabetes - this is really unexpected stuff.
comment by Steven Byrnes (steve2152) · 2020-03-26T17:19:47.005Z · LW(p) · GW(p)
I'm still trying to understand how COVID-19 actually spreads. (Related to my recent question on touching-vs-breathing [LW · GW].) Based largely on this article, my current very-low-confidence belief (in decreasing order of importance):
- Top transmission risk: Being near (2 meters) someone coughing ... or talking! Talking emits droplets / aerosols too. Is that the key to the pre-symptomatic transmission we know is happening [LW · GW]? Hmm.
- Second transmission risk: Air in or around public restrooms. Apparently a SARS carrier with diarrhea was a super-spreader, infecting people 200 meters away!! That same link also discusses evidence that COVID-19 virus is found around bathrooms.
- Last transmission risk: Touching contaminated surfaces then my face. While I am ranking this at the bottom, it could still be important, and I continue to take the same gung-ho precautions as when I formerly thought this was the primary thing to be thinking about [LW(p) · GW(p)].
Again, very low confidence in all this. Thoughts?
comment by Jan_Kulveit · 2020-03-09T23:56:33.360Z · LW(p) · GW(p)
We are looking for forecasters/"estimators" to help with estimating various COVID-19 parameters, such as number of infected cases, which will go into epidemic modelling, augmenting unreliable reported data. Ideally the end product should be the results of the modelling presented in a good web UI. If you would be interested in helping, reply privately.
Q&A: How does it compare to Metaculus? In a few important ways.
1. the estimates are not the end product, but an input to epidemic modelling software
2. in our UX, we want to clearly communicate the results of the epidemic are not pre-determined, but depend on actions humanity will take
3. we want to expose more of the uncertainties and underlying dynamic, as opposed to static forecasts
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-10T15:13:19.061Z · LW(p) · GW(p)
Have you thought about cooperating with Metaculus?
comment by Joel Chan (joel-chan) · 2020-03-18T17:47:20.651Z · LW(p) · GW(p)
Read the Imperial College COVID-19 Response Team report tonight. https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf
The numbers are quite starkly grim, based on an epidemiological simulation model. They conclude that mitigation strategies (only isolating symptomatic people, social distancing only at-risk people) will at best reduce the load on the healthcare system to "only" 8x current surge capacity in UK/US, leading to estimated 1.1M deaths from COVID-19 alone (i.e., not considering possible deaths from other causes due to an overloaded healthcare system). Instead, suppression strategies (everyone socially isolating) need to be followed for 12-18 months to ensure that the load from COVID-19 stays within surge capacity, minimizing total deaths to the low hundreds of thousands, and buying time for a vaccine / treatment to help beat back a second epidemic after relaxing suppression measures.
I am curious about a few assumptions in their model (wish it was open-sourced!), and how this might change the estimate.
1) They assume a fixed ICU capacity (where I think the main limit is ventilators, not just beds). Does anyone have any models/estimates of how much UK/US can expand intensive care capacity (e.g., with "wartime" style all hands on deck manufacturing and innovation)?
2) I don't see any modeling of social network effects in the mitigation scenarios. I'm thinking of the conjecture in this preprint (https://osf.io/fd4rh/?view_only=c2f00dfe3677493faa421fc2ea38e295) that intergenerational interactions, co-residence, and commuting patterns in Italy might have unique effects on the transmission and mortality rates.
Has anyone seen discussion of these points from experts? Or done some modeling themselves that could speak to these issues?
Also curious what others think of the report.
Replies from: Vaniver↑ comment by Vaniver · 2020-03-18T18:12:42.529Z · LW(p) · GW(p)
They assume a fixed ICU capacity (where I think the main limit is ventilators, not just beds). Does anyone have any models/estimates of how much UK/US can expand intensive care capacity (e.g., with "wartime" style all hands on deck manufacturing and innovation)?
My understanding is that the treatment requires significant monitoring and skill; the ventilation is often invasive (they have to get the tube into your lung, rather than just into your mouth).
But for a while people have been suggesting compartmentalizing the medical system further. If you just want someone to be a 'ventilator nurse', able to intubate a patient and then manage a ventilator for that patient, could you do that with a 30-day training program? Seems likely and worthwhile, but will require some sort of emergency legislation to authorize in most places, and some rapid development of curricula and testing.
Similarly, expanding production runs into legal issues. You may have heard about the volunteers who 3D printed ICU valves; they asked the company for blueprints, and the company threatened to sue for the IP violation. You might also have heard about the patent troll who sued the makers of a COVID19 test for infringement; they dropped the case once it was public that the use was a COVID19 test. It seems like a potentially sensible government action here is to nationalize (or otherwise force licensing) of technology that's useful in a disaster, with the government paying for the IP after-the-fact based on actual usage out of the overall disaster response fund.
But in general, our 'peacetime' standards for medical devices are very high. If you want to take your toaster factory (or w/e) and start spitting out ventilators instead, there's a lengthy approval process because this is complicated stuff with many ways things can go wrong. When the alternative is nothing, it's probably good to have rush jobs available, but there's nothing in place (that I'm aware of) to allow this sort of rapid ramping.
Replies from: leggi↑ comment by leggi · 2020-03-19T06:50:17.611Z · LW(p) · GW(p)
For intubation:
- The patient is usually sedated/unconscious. (drugs need to be administered)
- correct insertion of endotracheal tube ( endo ~ inside trachea = windpipe)
The first hard part is getting the tube past the vocal cords in the larynx. This requires the correct positioning of the patient to be able to see the vocal cords. (fibreoptic scope sometimes necessary) and to align structures for easier insertion.
Laryngospasm where the vocal cords come together to block the airway is a major concern. (the vocal cords coming together is a normal part of swallowing to prevent things going into the airways and contacting the cords will induce a spasm.) This can be reduced by using a local anaesthetic spray on the cords - essential if the patient is conscious (a rare situation).
Correct placement of the endotracheal tube is critical. It must be within the trachea, above the carina (where the trachea splits into the main bronchi and definitely not into a lung). If the tube goes into a bronchus it means one lung gets air, the other doesn't. A bad intubation is worse than no intubation.
For ventilation:
- Fancy equipment
or
- Someone squeezing a ventilation bag. (+ oxygen supplementation)
But ultimately, nurses/EMTs/medical students can be trained to do all this in a few days. If someone's competent and confident and has adequate back-up in-case of issues.
Replies from: Vaniver↑ comment by Vaniver · 2020-03-19T17:51:25.255Z · LW(p) · GW(p)
But ultimately, nurses/EMTs/medical students can be trained to do all this in a few days. If someone's competent and confident and has adequate back-up in-case of issues.
I think we might want to be in the world where we train a substantial fraction of the recently unemployed, or the National Guard, or whoever to do this, which requires starting from a lower point than nurses/EMTs/medical students.
↑ comment by leggi · 2020-03-20T08:05:48.780Z · LW(p) · GW(p)
There's a big difference between the process of intubation and maintaining a patient once intubated.
Someone with no prior knowledge of anatomy and physiology intubating patients (even after intense training) would increase the risks to patients. A mistake could be fatal. Time is a crucial factor - less than 4 minutes to correct an issue (brain needing oxygen).
Sedation/paralytic drugs need to be given. Dangerous in themselves. (an old saying re intravenous anaesthetics - dead easy, easily dead)
Adequate supervision/ back-up would be essential.
Aptitude of the trainee would also be very important. No room for getting stressed. 1st rule emergency medicine - breathe.
Better for the more experienced to intubate and then training people on ventilator management / how to squeeze a bag at the right pressure and timing (when ventilators aren't available).
↑ comment by leggi · 2020-03-20T08:15:46.463Z · LW(p) · GW(p)
Tracheal intubation in the ICU: Life saving or life threatening?
comment by ChristianKl · 2020-03-10T15:00:09.800Z · LW(p) · GW(p)
I know that a roommate of a friend if coughing regularly according to my friend. I'm living in Berlin. How likely is it that the roommate is having COVID-19 based on the available information? How careful should I be interacting with that friend?
comment by ignoranceprior · 2020-03-26T16:51:43.854Z · LW(p) · GW(p)
Epidemiologist Behind Highly-Cited Coronavirus Model Admits He Was Wrong, Drastically Revises Model (archive)
Epidemiologist Neil Ferguson, who created the highly-cited Imperial College London coronavirus model, which has been cited by organizations like The New York Times and has been instrumental in governmental policy decision-making, offered a massive revision to his model on Wednesday.
Ferguson’s model projected 2.2 million dead people in the United States and 500,000 in the U.K. from COVID-19 if no action were taken to slow the virus and blunt its curve.
However, after just one day of ordered lockdowns in the U.K., Ferguson has changed his tune, revealing that far more people likely have the virus than his team figured. Now, the epidemiologist predicts, hospitals will be just fine taking on COVID-19 patients and estimates 20,000 or far fewer people will die from the virus itself or from its agitation of other ailments.
Ferguson thus dropped his prediction from 500,000 dead to 20,000.
Author and former New York Times reporter Alex Berenson broke down the bombshell report via Twitter on Thursday morning (view Twitter thread below).
“This is a remarkable turn from Neil Ferguson, who led the [Imperial College] authors who warned of 500,000 UK deaths — and who has now himself tested positive for #COVID,” started Berenson.
“He now says both that the U.K. should have enough ICU beds and that the coronavirus will probably kill under 20,000 people in the U.K. — more than 1/2 of whom would have died by the end of the year in any case [because] they were so old and sick,” he wrote.
Thoughts on this?
Replies from: Wei_Dai, Lanrian↑ comment by Lukas Finnveden (Lanrian) · 2020-03-26T17:14:51.785Z · LW(p) · GW(p)
That article is based on a twitter thread that is based on this article that is based on the parliamentary hearing that Wei Dai linked. The twitter thread distorted the article a lot, and seems to be mostly speculation.
comment by jefftk (jkaufman) · 2020-03-09T15:40:43.233Z · LW(p) · GW(p)
I have a lot of hand sanitizer I bought for a dance weekend that is now cancelled. What should I do with it?
EDIT: I gave some to an immunocompromised friend, some to friends who have critical jobs, and the rest to a food pantry
Replies from: Gunnar_Zarncke, ChristianKl, pktechgirl, agc↑ comment by Gunnar_Zarncke · 2020-03-09T20:18:06.008Z · LW(p) · GW(p)
Keep them until you more clearly see what the best possible or most urgent immediate use turns out to be.
↑ comment by ChristianKl · 2020-03-09T19:32:47.370Z · LW(p) · GW(p)
How about donating them to nearby retirement home?
↑ comment by Elizabeth (pktechgirl) · 2020-03-09T17:09:42.269Z · LW(p) · GW(p)
Too bad ebay is no longer an option.
Replies from: FactorialCode↑ comment by FactorialCode · 2020-03-09T17:25:11.910Z · LW(p) · GW(p)
Facebook marketplace?
↑ comment by agc · 2020-03-09T15:45:22.941Z · LW(p) · GW(p)
Put them on a table at work or school with a sign saying "fee - take one".
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2020-03-09T16:23:15.596Z · LW(p) · GW(p)
I mean, I can definitely distribute them randomly. I'm trying to figure out if there's something better to do with them.
(They're also gallons, so a bit tricky to distribute)
Replies from: ady-jade-beacham↑ comment by Ŀady Jade Beacham (ady-jade-beacham) · 2020-03-09T19:14:20.634Z · LW(p) · GW(p)
If you are going to donate them I would suggest local hospitals or urgent cares might put them to best use.
I wish we had managed to get some hand sanitizer, we only managed to find travel sized ones before shtf.
Replies from: jimrandomh↑ comment by jimrandomh · 2020-03-09T21:23:41.425Z · LW(p) · GW(p)
Health care settings are likely to already be well supplied, and to be picky about which kind of hand sanitizer they use (even if it's just about getting an internal approval).
comment by Elizabeth (pktechgirl) · 2020-03-18T23:34:25.741Z · LW(p) · GW(p)
I was feeling rudderless trying to do actionable CV research without a grounding in its basic science, so I took a step back to build a foundation. These are the top sources that were useful to me:
- Medical Microbiology Chapter 57: Coronaviruses (less technical of the two, although still aimed at biologists)
- Coronaviruses: An Overview of Their Replication and Pathogenesis
These have also been added to the links DB
comment by IL · 2020-03-09T20:53:06.936Z · LW(p) · GW(p)
What's the best way to convince skeptics of the severity of COVID? I keep seeing people saying it's just a slightly worse flu, or that car accidents kill a lot more people, and so on. I want some short text or image that illustrates just how serious this is.
I found this heartbreaking testimony from an Italian ICU doctor: https://twitter.com/silviast9/status/1236933818654896129
But I guess skeptics will want a more authoritative source.
Replies from: steve2152, Lanrian, jdfaben, gwillen, ofer↑ comment by Steven Byrnes (steve2152) · 2020-03-10T16:28:18.134Z · LW(p) · GW(p)
A nice figure is that 1 person infected with COVID-19 requires (I think) 100x the hospital capacity of 1 person infected with the flu - 30x likelier to need hospitalization, and they stay there 3x longer if they do (you'll have to check these figures, but it's something like that I think...). Then that connects to the nightmarish Italian hospital situation you mention, and the fact that the death rate is dramatically higher without available hospital beds, including for young healthy people [LW(p) · GW(p)].
↑ comment by Lukas Finnveden (Lanrian) · 2020-03-11T21:09:36.931Z · LW(p) · GW(p)
Angela Merkel says that 60-70% of Germany is likely to be infected. That's useful if people believe that it won't infect that many. Example source, though you can google for others.
If they're willing to believe a redditor's summary, this one says that WHO says that 20% of infected people needed hospital treatment for weeks. (If they want primary sources, maybe you could find those claims in the links / somewhere else.)
Putting together 1 and 2 (and generalising from Germany to whatever country they're in), they ought to be convinced that it's pretty severe.
↑ comment by jdfaben · 2020-03-16T10:57:10.797Z · LW(p) · GW(p)
It is now literally not true that car accidents kill more people, in either the UK or Italy, and won't be true in the US in about a week.
I've found the time-delayed log graphs like this one pretty convincing: https://images.app.goo.gl/iKrfzw9Wt7hAqkVB6
↑ comment by gwillen · 2020-03-09T23:43:49.120Z · LW(p) · GW(p)
For today, I have been directing people to this chart of Italian intensive care hospitalizations and deaths, 2020 COVID-19 vs 2018-2019 flu season: https://twitter.com/DellAnnaLuca/status/1236805732525207552
(Source: http://www.biotecnologi.org/ecco-perche-il-coronavirus-non-e-una-semplice-influenza/)
As well as this news story about Italy banning all public gatherings across the whole country: https://www.bbc.com/news/world-europe-51810673
Plus the fact the the stock market is down >10% over the last week...
↑ comment by Ofer (ofer) · 2020-03-10T15:11:51.615Z · LW(p) · GW(p)
Maybe citing the CDC:
It’s likely that at some point, widespread transmission of COVID-19 in the United States will occur. Widespread transmission of COVID-19 would translate into large numbers of people needing medical care at the same time. Schools, childcare centers, and workplaces, may experience more absenteeism. Mass gatherings may be sparsely attended or postponed. Public health and healthcare systems may become overloaded, with elevated rates of hospitalizations and deaths. Other critical infrastructure, such as law enforcement, emergency medical services, and sectors of the transportation industry may also be affected. Healthcare providers and hospitals may be overwhelmed. At this time, there is no vaccine to protect against COVID-19 and no medications approved to treat it.
comment by TurnTrout · 2020-03-09T05:25:14.001Z · LW(p) · GW(p)
Should poly people consider stopping intimate contact (hugs+) at some point? The network structure of polyamorous relationships might make people particularly vulnerable.
Replies from: MaxCarpendale, ady-jade-beacham↑ comment by MaxCarpendale · 2020-03-14T20:48:22.277Z · LW(p) · GW(p)
Having all partners isolate together is maybe another option for small polecules who all get along well.
↑ comment by Ŀady Jade Beacham (ady-jade-beacham) · 2020-03-09T19:07:23.739Z · LW(p) · GW(p)
Household transmission In China, human-to-human transmission of the COVID-19 virus is largely occurring in families. The Joint Mission received detailed information from the investigation of clusters and some household transmission studies, which are ongoing in a number of Provinces. Among 344 clusters involving 1308 cases (out of a total 1836 cases reported) in Guangdong Province and Sichuan Province, most clusters (78%-85%) have occurred in families. Household transmission studies are currently underway, but preliminary studies ongoing in Guangdong estimate the secondary attack rate in households ranges from 3-10%.
From the WHO report on China, most infection clusters they found were family clusters. This may be applicable to your thinking on this.
Replies from: jimrandomh↑ comment by jimrandomh · 2020-03-09T21:10:01.629Z · LW(p) · GW(p)
Something is weird about that 3-10% secondary attack rate number. The study isn't published yet, so I don't know what exactly they're measuring, but I'm pretty confident that people who share a household and hug each other will transmit at much greater than 10% probability.
Replies from: gwillen, gwillen↑ comment by gwillen · 2020-03-16T00:40:24.219Z · LW(p) · GW(p)
This is a fairly late update, but closing the loop on this: I believe the 3-10% number ended up being the secondary attack rate among households where the infected person was isolated after diagnosis. So that's an estimate of the rate of transmission during extended close contact before symptoms/diagnosis, not after, which makes more sense. I assume that extended close contact with a symptomatic infected person will result in very likely transmission.
↑ comment by gwillen · 2020-03-09T23:30:03.169Z · LW(p) · GW(p)
Keep in mind that there may be substantial variation in the amount of viral shedding for infected people (there are superspreaders, presumably there are also subspreaders), as well as in the susceptibility of people to the virus (presumably there is some cross-immunity for people who have had a coronavirus-type common cold recently, for example.) So the transmission rate among household members can't necessarily be estimated from the per-contact rate assuming each contact is an independent chance of transmission.
comment by Isnasene · 2020-03-30T22:58:00.101Z · LW(p) · GW(p)
[Epistemic Status: It's easy to be fooled by randomness in the coronavirus data but the data and narrative below make sense to me. Overall, I'm about 70% confident in the actual claim. ]
Iran's recent worldometer data serves case study demonstrating relationship between sufficient testing and case-fatality rate. After a 16 day long plateau (Mar 06-22) in daily new cases which may have seemed reassuring, we've seen five days (Mar 24-28) of roughly linear rise. We could anticipate this by noticing that in a similar time frame (Mar 07-19), we were seeing a linear rise in case fatality rate before it became constant. This indicates the following narrative (not sure if it's actually true):
- Coronavirus spreads uncontrolled in Iran without increased testing capabilities. This causes new daily cases to stay constant despite increased infection -- the 16 day long plateau in daily new cases
- Because cases are increasing, the number of severe cases is also increasing - - and severe cases are more likely to get tested than less severe cases. This causes fatality rate to rise as the severity of the cases that are actually tested increases -- the 12 day linear rise in case fatality
- Recently, testing capabilities were ramped, allowing testing of more people and the observation of less severe cases. As a result, the number of daily cases started increasing again with the testing rate. Simultaneously, the fatality rate plateau'd as the (complex) trend in severe cases being tested in greater proportion to less severe cases was cancelled out by trend in testing. Hence the last five days of daily new case rise and the past eight days of constant fatality rate.
- Note that this narrative suggests that testing is being continuously ramped up while remaining the bottle-neck. Two pieces of evidence for this:
- The daily cases start increasing linearly from the plateau. If testing was increased dramatically, one would an immediate discontinuous increase in number of daily cases at the point where more tests are done.
- Iran's death rate is still much higher (17% compared to an IFR which should be less than 5%) so testing is unlikely to be sufficient to capture the true infection rate
comment by DanielFilan · 2020-03-14T20:32:15.179Z · LW(p) · GW(p)
Metaculus has extended the Li Wenliang prize series - win $$$ as well as internet points by forecasting the course of the COVID-19 pandemic!
Replies from: DanielFilan↑ comment by DanielFilan · 2020-03-15T22:28:38.642Z · LW(p) · GW(p)
And the prize money for the second installment has increased since I wrote this comment!
comment by Ben Pace (Benito) · 2020-03-17T23:22:04.747Z · LW(p) · GW(p)
Today will always be the day that, for one hour, Facebook removed all posts/comments that had links to any of The Atlantic, Medium, and LessWrong. Because we're just that big and important.
(The issue is now fixed.)
comment by PeterMcCluskey · 2020-03-16T04:04:39.759Z · LW(p) · GW(p)
Here's some perspective on U.S. stock market reactions to bad news (of nonfinancial origins):
- 1918 Spanish Flu: -10% in slightly over 5 weeks?
- 1940 Fall of France: -25% in slightly over 2 weeks
- 1942 Pearl Harbor: -11% in slightly over 3 weeks
- 2001 9/11: -12% in less than 2 weeks
- 2020 COVID-19: -26% in 3 weeks (so far?)
These numbers are based on closing values for the S&P500 (for 1918: the DJIA), from the day before the obvious start of the crash, to an obvious low point where it stabilized. Note that the reaction to the 1918 flu is confusing, maybe because WW1 ended just as the biggest wave of the flu ended. The big increase in death rates in New York started around October 1, and peaked in late October. Yet the DJIA was higher in late October than on October 1. I've calculated the decline from the October 18 peak to the November 25 low, but I don't think it took that long to finish reacting to the flu.
My intuition is that COVID-19 will cause no more harm than 9/11 or the 1918 flu. Why does the market act like this is slightly worse news than the Nazi occupation of France? It's not due to problems that are specific to the U.S. - many European markets are doing worse.
Yet the Shanghai Composite is down less than 8% from it's January high, and is above its early February low.
Maybe the U.S. and European markets had reflected a much safer world than anyone at the time of prior disasters had expected?
Replies from: maia, romeostevensit, FactorialCode↑ comment by maia · 2020-03-16T15:52:11.029Z · LW(p) · GW(p)
Complete speculation here: Our economy in 1918 was based much more on agriculture and industry, whereas now it is much more based on services, aka people going to work, which they now can't do, and also much larger. So perhaps the coronavirus will, in fact, destroy more real value than the Spanish flu was able to, even as a percentage of the market.
↑ comment by romeostevensit · 2020-03-19T01:15:42.633Z · LW(p) · GW(p)
>Maybe the U.S. and European markets had reflected a much safer world than anyone at the time of prior disasters had expected?
that's part of what super low rates/yield imply right? That people expect a very stable world. Higher multiples are flimsier in the face of new evidence.
↑ comment by FactorialCode · 2020-03-16T05:23:00.877Z · LW(p) · GW(p)
There are probably many factors that make this different now than before. However, I suspect that markets today are just smarter than back then. As a result, they react much quicker to information than before. I don't think you can estimate the drop magnitude by the looking solely at the rate of decrease.
comment by SoerenMind · 2020-03-15T15:18:06.181Z · LW(p) · GW(p)
1/13 people have Asthma. How much worse off are we?
Replies from: SoerenMind↑ comment by SoerenMind · 2020-03-17T17:28:24.174Z · LW(p) · GW(p)
Data point: There were no asthma patients among a group of 140 hospitalized COVID-19 cases in Wuhan.
But nobody had other allergic diseases either. No hay fever? Seems curious.
Replies from: jkaufman, pktechgirl↑ comment by jefftk (jkaufman) · 2020-03-18T00:39:49.267Z · LW(p) · GW(p)
Allergies and asthma are rare in China and other poorer countries. The standard explanation I'vev head is https://en.wikipedia.org/wiki/Hygiene_hypothesis
↑ comment by Elizabeth (pktechgirl) · 2020-03-17T17:48:39.606Z · LW(p) · GW(p)
That group also was only 1.4% smoker, while china-normal in 2015 was 27.7% (almost all of whom were men). I wonder if people worried they'd get worse care if they admitted to respiratory co-morbidities?
Replies from: SoerenMind↑ comment by SoerenMind · 2020-03-18T02:42:52.688Z · LW(p) · GW(p)
Right now I expect they just used hospital admission forms. If I was self-reporting 5 pages of medical history while I'm critically ill I'd probably skip some fields. Interesting that they did find high rates of diabetes etc though.
comment by Chris S · 2020-03-15T06:27:11.832Z · LW(p) · GW(p)
Here's a credible-seeming claim from a computational biologist that, if COVID-19 is like other coronaviruses, long term immunity is unlikely. I imagine this also means a vaccine is unlikely.
If true, this changes everything. Does this mean we are all going to be working from home for the rest of our lives? Or will we accept a world where there is an endemic disease that we get for 3 weeks every year?
Replies from: gwillen↑ comment by gwillen · 2020-03-16T00:44:19.499Z · LW(p) · GW(p)
I think this doesn't quite change everything, for the following reasons:
- Even if long-term immunity is unlikely, short-term immunity will push this back towards the flu category, where most people are not getting it acutely at the same time. This will significantly improve the healthcare situation vs what we're seeing in the pandemic phase.
- Diseases evolve towards increased spread, which usually involves evolving towards reduced lethality / severity. If this becomes endemic it's likely to do the same.
- If it turns out that this does become a severe endemic disease, there will be a lot of pressure on the development of a vaccine, much more so than has been true for human coronaviruses in the past (when they were much closer to being mostly a nuisance, and included in the general "common cold" category.) Even if long-term immunity is unlikely, we can still improve the situation like we currently do with influenza, giving people periodic boosters based on the current circulating strains.
↑ comment by Chris Hibbert (chris-hibbert-1) · 2020-03-22T18:19:49.358Z · LW(p) · GW(p)
Diseases normally evolve toward increased spread by reducing lethality because they don't have a superpower like Covid2019's ability to spread while the carrier is asymptomatic. I don't think there's much evolutionary pressure on this disease toward lower severity. Even if we do a good job of enforcing shelter-in-place in populous areas, there will be hidden reservoirs until we reduce the number of new cases in connected communities all the way to zero.
The normal evolutionary pressure works because there's some variation between different strains, and whichever variant can reach the most people comes to dominate. With a normal infection, once everyone is aware, you can quarantine people with evident symptoms and thus squelch the spread. Any variant that has milder symptoms has a better chance of spreading and becoming dominant. Covid2019 already has the ability to escape surveillance if there's any of it in the population, so a less lethal variant doesn't have a selective advantage.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2020-03-22T19:38:04.060Z · LW(p) · GW(p)
My understanding is that asymptomatic spread is pretty common.
↑ comment by Chris S · 2020-03-16T02:39:17.294Z · LW(p) · GW(p)
That's a good answer, and consistent with this very good article by Johns Hopkins epidemiologist Justin Lessler. He makes many of the same points you make, and adds that there will likely also be partial immunity even within individuals. (At least, I suppose, if we aren't facing antibody-dependent enhancement.)
comment by gwillen · 2020-03-12T01:13:56.163Z · LW(p) · GW(p)
A friend of mine (who lives in the SF Bay Area, currently somewhat of a coronavirus hotspot) posted to Facebook that he hasn't been feeling well recently and he thinks he might be sick (and was having trouble focusing at work yesterday). I posted the following; I don't know him well enough to know how he'll take it, but we'll see. I feel like we're still at a point on the curve where this kind of individual outreach can potentially have substantial value, so I'm offering it as perhaps a template for other people to use.
Yikes, good luck -- I hope you feel better!
If you can, please consider staying home from work and other events. Santa Clara County is a coronavirus hotspot right now, and we need everybody who is able to help reduce the spread. (That doesn't mean you have it, but you very much could.)
If it is the coronavirus: most cases (~80% average, but more than that in younger people, and people without major preexisting conditions) will resolve on their own without treatment; but if you do need medical attention, make sure you call ahead first. I believe self-quarantine is recommend until end of symptoms plus 24 hours, but there is evidence of viral spread until up to 10 days after start of symptoms, so I would suggest whichever is later. "Secondary attack rate" -- that is, the rate of spread to close contacts -- has been estimated at up to 10% for family/household members, so keep that in mind.
Please let me know if there's any more information I can provide or anything I can do to help.
comment by Eli Tyre (elityre) · 2020-03-11T06:34:40.859Z · LW(p) · GW(p)
Does anyone have updated figures on the fatality rate for different age groups, compared to the ones posted in this [LW(p) · GW(p)] comment?
I imagine that that table is mostly based on data from the early outbreak in China, which may or may not generalize well to say, my parents.
Replies from: christoph-richter↑ comment by Christoph Richter (christoph-richter) · 2020-03-12T00:22:46.016Z · LW(p) · GW(p)
https://www.tableau.com/about/blog/2020/3/covid-19-resources-data-viz-best-practices
This provides a more detailed overview of the china data.
Specially, most patients have been ill before. As Cadiovascular conditions mostly are with elderly persons this makes them a high risk group.
comment by ignoranceprior · 2020-03-20T06:03:30.864Z · LW(p) · GW(p)
Questions about buying chloroquine:
1. Is it better to buy hydroxychloroquine or regular chloroquine? The studies I've found suggest hydroxychloroquine is safer and more potent, but it is a bit more expensive.
2. How many days worth of the drug is it reasonable to buy per person?
3. How much should someone take per day and how should the dosage be timed?
4. Can someone confirm that the products you can find on reliablerxpharmacy.com when searching for "Lariago" (500 mg chloroquine as phos) and "OXCQ" (200 mg Hydroxychloroquine Sulfate) are the right things to buy? If not, is there any other reputable or semi-reputable source that sells the right product?
Replies from: johnlawrenceaspden↑ comment by johnlawrenceaspden · 2020-04-07T10:23:14.444Z · LW(p) · GW(p)
That's the right stuff I think (chloroquine phosphate, very bitter tasting), would you say that reliablerxpharmacy is a good and trustworthy source?
(not for chloroquine, for meds generally without a prescription)
comment by TobyBartels · 2020-03-15T18:12:11.708Z · LW(p) · GW(p)
Hi, I haven’t posted in a while, and I hope that people are still reading new comments in this thread, because I need an answer fast, and this is the best place that I know to get a good one. (Well, second best. I posted to SSC first.)
My parents, age 70, live in Lincoln NE (population 285 thousand, no reported cases of Covid-19 yet, 17 reported cases in the State, schools just closed and are preparing to go online). They pretty much run their bridge club, most of whose members are in their 70s but generally in good health. The club has an event planned for tonight (March 15 Sunday), at which 26 people are expected to show up and sit at card tables in close proximity, moving from table to table over the course of the evening. There will be hand sanitizer available at the tables.
Question: Should they cancel the event?
Please give reasons for your answer as if you’re trying to convince a stubborn Boomer (but not a Trump-supporter). You may assume that your audience is mathematically literate. If you know any data on age-related risks that controls for other risk factors, then that would be a big bonus. (Because since heart disease, diabetes, and lung disease are all risk factors for Covid-19, and since they’re also all more prevalent among older people, maybe age alone is not much of a risk factor all.)
Replies from: pktechgirl, TobyBartels, pktechgirl, TobyBartels↑ comment by Elizabeth (pktechgirl) · 2020-03-15T18:32:50.459Z · LW(p) · GW(p)
Here is what I wrote my dad in attempt to get him to close up the church of which he is an elder, in a similarly sized city. My dad is a statistician and 30% prepper, so this was more about giving him evidence to take to others than convincing him:
I made a model to translate deaths in an area into probable number of current infections, and another to make a crude guess at what prevalence hospitals will be over-capacity (the answer is 1.5%). Based on my math, 1 confirmed death in [county] implies a prevalence of 0.13% (range 0.027% to 0.43%), which is 4 doublings away from overwhelming hospitals. However the doubling time is also used to calculate the current prevalence, so if you think the doubling time is very short you not only have very little time from .1 to .2%, but you're more likely to already be at .3%. So in the 5th percentile scenario you're at .43% and have only 6 days until you're over 1.5%.
I think people should quarantine themselves at least three weeks before their municipality reaches hospital saturation (so that if they get it, it's before the peak). So under the current testing regiment, a single confirmed community transmission case in [county[ should absolutely trigger a shut down. If we get decent survey testing system going it would of course be different.
The other thing to watch out for is excess pneumonia deaths. I don't know how to check this, but if there's a noticeable bump in pneumonia I would attribute them all to COVID-19.
I didn't think of this at the time, but in retrospect it would have been helpful to suggest replacements for an in-person service. I'll bet it is easier to convince your parents' friends to switch to online bridge with voice chat than to give it up entirely.
↑ comment by TobyBartels · 2020-03-16T17:42:38.998Z · LW(p) · GW(p)
I have good news and bad news. The bad news is that the game went on last night as planned. The good news is that my parents won't be attending any more large games. The bad news is that there are still going to be more large games, at least one tonight. Although it's mostly the same population every time.
Replies from: TobyBartels↑ comment by TobyBartels · 2020-03-17T21:22:53.866Z · LW(p) · GW(p)
The club is now closed until further notice.
↑ comment by Elizabeth (pktechgirl) · 2020-03-16T03:46:22.745Z · LW(p) · GW(p)
↑ comment by TobyBartels · 2020-03-15T20:06:42.714Z · LW(p) · GW(p)
Previous versions of this question: https://slatestarcodex.com/2020/03/11/open-thread-149-25/#comment-865412 https://slatestarcodex.com/2020/03/15/open-thread-149-5/#comment-865535
comment by Bucky · 2020-03-14T10:22:39.875Z · LW(p) · GW(p)
I have created the top two graphs of my previous post [LW · GW] on outbreak speeds as interactive versions here (thanks to Ruby for helping with getting this uploaded). The labels on the right are clickable to remove or add countries (double click selects only that country or all countries). The buttons at the top change the y-axis (annoyingly the y-axis range buttons auto-set to a linear scale) and the slider at the bottom zooms the x-axis.
comment by MaxCarpendale · 2020-03-13T19:37:39.701Z · LW(p) · GW(p)
We started an effective altruist coronavirus discussion group on Facebook and there are a lot of posts in it. The link is here if you're interested.
comment by James_Miller · 2020-03-11T01:55:42.352Z · LW(p) · GW(p)
From a friend who is a microbiologist Phd "Oh and drink plenty of water. My lab group discovered that humans and cows partially rid their body of viruses (at least adenovirus) through their urine. "
Replies from: romeostevensit↑ comment by romeostevensit · 2020-03-12T01:52:44.435Z · LW(p) · GW(p)
It also apparently helps with lessening the spread from the mouth/throat to the respiratory tract making it more likely to stay mild.
comment by jimmy · 2020-03-18T20:26:51.831Z · LW(p) · GW(p)
The one situation where an entire, closed population was tested was the Diamond Princess cruise ship and its quarantine passengers. The case fatality rate there was 1.0%, but this was a largely elderly population, in which the death rate from Covid-19 is much higher.
Projecting the Diamond Princess mortality rate onto the age structure of the U.S. population, the death rate among people infected with Covid-19 would be 0.125%.
John Ioannidis is making an interesting (and reassuring, if true) claim here. Has anyone looked at the demographics and done the comparison themselves?
Replies from: Lukas_Gloor, Roko↑ comment by Lukas_Gloor · 2020-03-18T21:51:21.936Z · LW(p) · GW(p)
This can't be right. I've looked into Diamond cruise studies and some stay at 1% even after adjusting for age (they factor in that more people might have died in the meantime – even though that didn't happen so far, admittedly – and the unadjusted number is 1% at least already; makes you wonder whether elderly cruise goers are healthier than their stay-at-home cohorts). I've found this study which, after doing some adjustment steps I don't understand but find dubious (maybe they double adjusted something by accident?), ends up estimating 0.5% for China's total outbreak. You might think this makes the 0.125% figure mentioned by Joannidis somewhat plausible, because China's outbreak had a majority of cases in Hubei where patients didn't all have access to hospital care. This is likely to drive up the fatality rate. However, the study didn't account for that. They just implicitly assumed that people who got sick on the cruise ship had the same prospects as people who got sick in China. And they may or may not have halved their estimates in some dubious way too. So, 0.5% seems like an absolute lower bound here, and more likely it's higher. 0.125 is extremely implausible if you ask me.
UPDATE: I did some calculations for age adjustments on the Diamond Princess here [LW(p) · GW(p)] and I now consider it to be only weak evidence against a 0.125% estimate. My own age adjustment returned a point estimate of about 0.2%, which I argue should be further adjusted upward for reasons related to selection effects of the type of people who go on cruises.
In addition, South Korea now has a 1% CFR. They've done >230,000 tests, sometimes more than 10,000 tests per day. They only have about 8,500 confirmed diagnoses, so with the number of tests that they're doing, one would assume that they caught most of the illnesses. I think they even must have caught most of the asymptomatic cases, because a large portion of their diagnoses was from this Christian sect (which happens to have a young demographic too), and I think they tested almost everyone on their membership records.
Finally, the Imperial College experts who advise the UK government recently revised their estimates and gave out a 0.9% infection fatality rate estimate (see page 5 mostly). This presumably applies to favorable conditions rather than hospital overstrain. Edit: In the 80k podcast Howie Lempel said it's a prediction about what's likely to hit the UK. He might be right and if that's the case, it would factor in some degree of hospital overstrain.
All of this strongly suggests that Joannidis is spreading dangerous misinformation. But maybe there's something I and others are not seeing.
Replies from: jimmy↑ comment by jimmy · 2020-03-19T01:41:00.207Z · LW(p) · GW(p)
Yeah, the 1/8th multiplier sounded hard to believe. A 1/2 multiplier based on demographic correction sounds a lot more plausible, and it's nice to have confirmation that someone else actually did the math. Thanks for finding/sharing it!
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2020-03-20T16:34:16.355Z · LW(p) · GW(p)
I should flag that I didn't do the math for age correction. I only got this from another Diamond cruise study where the age correction provided a smaller update (and I didn't really like other things about that study).
So, I think it could be valuable to investigate this claim more:
Projecting the Diamond Princess mortality rate onto the age structure of the U.S. population, the death rate among people infected with Covid-19 would be 0.125%.
(But even if this point was right, there's still South Korea to explain.)
Replies from: Lukas_Gloor, jimmy↑ comment by Lukas_Gloor · 2020-03-20T19:43:59.598Z · LW(p) · GW(p)
Reading the Ioannidis article, it seems to say that he did his own calculations, and he doesn't show them. Okay.
I'm curious about this, so I'm going to try a ballparking estimate myself.
Tl;dr I intially arrived at a result that suggested 0.125% was way off, but then found better info on the cruise ship's age distribution and had to revise my judgment. I now find it debatable whether 0.125% is defensible or not, but it's not "way off." My own estimate would be more in the ballpark of 0.3%, but I don't anymore consider the cruise ship to be evidence for IFR estimates at 0.5% or higher.
Update March 24th: In the couple of days, 3 new patients who had tested positive on the Diamond Princess have died. In addition, the Wikipedia article has been edited to list another death that previously hadn't been included. So total deaths per confirmed cases on the Diamond Princess are now 11 / 700 instead of 7 / 700. All my calculations below are based on the older, outdated numbers. To get the most updated estimates, just multiply the results below by 11/7.
---
Note that I have never done age adjustments for anything, so I have no idea what the proper methdology would be. I'm just curious to see if 0.125% is potentially reasonable rather than (as my current intuition suggests) very dubious.
From this paper, I found the following info:
A total of 634 people tested positive among 3,063 tests as at 20 February 2020. Of 634 cases, a total of 313 cases were female and six were aged 0–19 years, 152 were aged 20–59 years and 476 were 60 years and older.
At the end of the outbreak, roughly 700 people had tested positive. I'm going to assume that the 66 patients not yet in the above statistics fall into age categories in the same proportion. So a bit more than two thirds of the 66 patients get added to the 476 figure for people aged 60 and older.
With this adjustment, we have 700 diagnosed cases, of which an estimated 525 patients were aged 60 and older. Of those 700 diagnosed cases, 7 people died. 525 out of 700 corresponds to 75%. (I'm going to mostly ignore the death risk for people below age 60 for the analysis below, because it will be negligible given that people older than that anyway make up the majority share.)
This wikipedia article on US demographics says the following:
- 0–14 years: 18.62%
- 15–24 years: 13.12%
- 25–54 years: 39.29%
- 55–64 years: 12.94%
- 65 years and over: 16.03%
Eyeballing this, let's go with 22% of the population at age 60 or older.
75 divided by 22 is roughly 3.4, so this naively suggests that the cruise ship's demographic was roughly 3.4 times more susceptible to dying from SARS-CoV-2. If I divide the observed IFR of 1% by 3.4, I get 0.3%. Why does Ioannidis get 0.125% instead of 0.3?
Moreover, it seems to me that 0.3% must be an underestimate because I assume that even though the cruise ship population is substantially older on average than the US population, I would think that this effect will disappear (or even reverse) at the extremes, once we look at the percentage of exceptionally old people (e.g., aged 80 and above, age 85 and above, etc.). Because Covid-19 is particularly fatal for the very oldest people, I expect the 0.3% figure to contain a substantial degree of overcorrection. Especially also because elderly people with the most severe pre-existing health conditions are likely heavily underrepresented on cruise ships. This effect could be really quite significant: It's not even totally obvious that a downward adjustment of the 1% IFR observed on the Diamond Princess is warranted. It's probably warranted, but depending on how strongly cruise ship passengers are pre-selected against having unusually bad health, and depending on how strongly pre-existing health conditions affect someone's survival prospect for Covid-19, it's conceivable that the 1% figure doesn't need to be downward adjusted at all.
To conclude, I don't understand how age adjustments for SARS-Cov-2 infections on the Diamond Princess can drive down the estimated IFR substantially below 0.5%. 0.5% seems closer to a lower bound to me than anything else. (Of course, those are point estimates. I don't have strong views on whether 0.125% is outside some appropriate confidence interval, but my impression was that 0.125% was Ioannidis's point estimate, and interpreted as such, it seems clearly much too low!)
UPDATE: Oh I see. I found an age table that I had overlooked initially. It turns out cruises are really popular for people at age 70-79 (there are about 20% more people of that age than 60-69, whereas it's the other way around for US demographics). This distribution makes Ioannidis's figures look more plausible, though the difference doesn't seem large enough to fully bridge the gap between 0.3% and 0.125%, especially because the 80-89 bracket seems to be represented proportionally again. Still, I don't anymore think that 0.125% is horribly off.
Replies from: ErickBall↑ comment by ErickBall · 2020-03-21T16:20:03.457Z · LW(p) · GW(p)
You found an age distribution for the infected population on the Diamond Princess, but you're using it as if it's the age distribution for everyone on the ship. Older people are more likely to get infected, so the infected population in the US will lean older as well--closer to the distribution on the ship. To do a good age adjustment we need to know the ages of the people on the ship who were not infected.
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2020-03-21T17:17:48.536Z · LW(p) · GW(p)
Older people are more likely to get infected, so the infected population in the US will lean older as well--closer to the distribution on the ship.
Interesting! Do you think this is established? I haven't looked into this, but my guess would have been that the risk is similar because young people are less scared of the virus. But yeah, good point about further adjustments being needed to get the best estimate.
Replies from: ErickBall↑ comment by ErickBall · 2020-03-22T05:40:01.020Z · LW(p) · GW(p)
Hmm, maybe you're right. The South Korean distribution of cases by age here suggests that it's actually most common by far among people in their twenties, and the larger number of confirmed cases among older people is a statistical artifact resulting from test criteria. The data do look a bit suspicious though.
↑ comment by Roko · 2020-03-18T21:06:15.432Z · LW(p) · GW(p)
I don't think the view in that piece here is consistent with what happened in Lombardia in Italy, but I haven't seen a detailed numerical argument against it.
Replies from: Lukas_Gloor↑ comment by Lukas_Gloor · 2020-03-20T20:19:34.262Z · LW(p) · GW(p)
I also thought that in Lombardia, the estimates given by Ioannidis are rapidly trending toward coming in contradiction with SIR models. :( Lombardia has a population of 11 million people and 2,500 reported deaths. Some doctors are raising alarm that many deaths are going undetected because people are dying at a rate that's 4 times higher than the same month last year. In addition, the death counts always lags behind because some people are sick for a long time before they die (though maybe this start to be the case less strongly in conditions of extreme hospital overstrain). All of this suggests that an estimate of 10,000 deaths for Lombardia alone might soon prove to be accurate. But according to the IFR provided by Ioannidis, this would correspond to an expected 8 million people infected (72% of the population). I don't understand SIR models well enough to calculate what the R0 would have to be for 72% of a population to get infected. I suspect that Covid-19's R0 is high enough to be consistent with this, but it wouldn't leave a lot of room for estimation errors.
That said, I think the above calculation is naive, so the argument doesn't work (at least not in this crude form). If hospitals become as overwhelmed as they are in Italy, I'm sure that even someone with Ioannidis' view would expect the IFR for Lombardy to become a lot higher than 0.125% because a lot of people aren't getting life-saving hospital attention.
So, this means that Lombardy isn't necessarily a knockdown argument against Ioannidis's estimate in the same way South Korea is. However, I think Ioannidis's estimate would have counterintuitive implications for the percentage of people infected in Lombardy. It would have to be in the double digits already at the very least. The most trustworthy estimate I saw about Wuhan suggested that only 5% of its population had the virus. However, there's some disagreement about this, and the people who tend to argue for an unusually low IFR also tend to argue that there's a giant iceberg of undetected asymptomatic cases.
UPDATE: I just realized something: I read somewhere recently that Italy is doing 30,000 tests a day by now, and that about 25% of them are positive. This seems to be in contradiction with Ioannidis's estimate because his view should imply that, if there's some kind of selection at all for who they are testing (as opposed to just testing members of the population at random), then we should expect to see more positive test results than 25%. (Why? Because if we assume that hospital overstrain increases his death rate estimate by a factor of 7x (which is a really large adjustment!), the death count estimates for Lombardy combined with Ioannidis's estimates would still suggest that above 10% of the population would have the virus. Such high numbers would only be consistent with reality if most people had relatively mild symptoms or no symptoms at all, so assuming that there's substantial pre-selection on who is getting tested (as opposed to random testing, which would be odd), a rate of 25% positive tests would be implausibly low for the scenario where >10% of the region were infected. So, to conclude, I think one can plausibly construct a case against Ioannidis's estimates based solely on common sense and numbers from Lombardia. I probably haven't quite succeeded at making this case in a watertight way, but I think you might be right with your intuition. This is just one more reason why the 0.125% estimate is completely absurd.
comment by qirlib (kirill-belov) · 2020-03-12T18:54:22.380Z · LW(p) · GW(p)
Does this thread welcome asking for highly personalized advice? I'm stuck with a few possible action options and the explanation is quite lengthy and the answers will probably be relevant to very few. I can't decide whether this thread is only about posting globally useful things or not.
Replies from: pktechgirl, Raemon↑ comment by Elizabeth (pktechgirl) · 2020-03-13T00:20:35.142Z · LW(p) · GW(p)
That would be discouraged in a top level post but is exactly the kind of thing this post is for.
comment by RedMan · 2020-03-11T04:04:20.761Z · LW(p) · GW(p)
In the usa, much of the workforce is paycheck to paycheck and does not have paid leave or short term disability, and health issues are a common cause for bankruptcy. So the following is applicable to a lot of people who probably are not in this (rationalist/lesswrong) community:
If you don't work, you don't get paid, so you don't make rent. If you get quarantined by the state after a positive test, you don't go to work, you don't get paid, and you don't make rent. If you don't make rent, you probably will not have a place to live. If you end up in the hospital, you will probably go bankrupt, and may not have a place to live when you get out. Therefore with the incentives in front of you, take the following advice: 'do as you would normally, go to work no matter how you feel, do not under any circumstances get a coronavirus test, as that might provoke some authority to put you in a position where you cannot get paid.' This is particularly relevant if you live in a state that decides to be aggressive and punitive about quarantining.
Walmart appears to have realized this and is taking measures to adjust the incentives, but it's probably too little too late.
I also expect red states to adopt punitive legislation and pundits representing those communities to not understand why it makes things worse (I've seen right wing blog comments that go something like this: hurr in the days of bubonic plague communities in Italy bricked up houses around infected families, we r not hard enough nowdays durrr).
For the rest of us, recognize that when you interact with a gig worker or any other member of the public with those incentives, they have a high risk of exposure from the community, are unlikely to use PPE (not part of the uniform, not affordable, etc), and regardless of whether they are showing symptoms, will probably work until either prohibited from doing so, or physically unable to due to symptoms.
I'd prefer to live in a community that took effective large scale action (lock down access to vulnerable groups, mass test the healthy, and create strong incentives to self-isolate), but I don't so whatever.
comment by James_Miller · 2020-03-09T22:51:11.047Z · LW(p) · GW(p)
I have been taking NAC (n-acetylcysteine) as a supplement for a while. You can (still) buy it on Amazon. From an Elsevier press release "The authors draw attention to several randomized clinical studies in humans that have found that over the counter supplements such as n-acetylcysteine (NAC), which is used to treat acetaminophen poisoning and is also used as a mucus thinner to help reduce bronchitis exacerbations, and elderberry extracts, have evidence for shortening the duration of influenza by about two to four days and reducing the severity of the infection". Anecdotally, I stopped taking NAC for a few months and happened to catch a cold. The phlegm took longer to go away than normal and I happened to read that NAC, which I still had, helped with phlegm, so I started taking NAC again and my phlegm problem quickly went away, at a faster rate than it had been.
comment by Raemon · 2020-03-08T23:53:33.337Z · LW(p) · GW(p)
I'm particularly interested in people sharing models / spreadsheets that they're currently working through here. (Posting them as top level posts is also fine, but I thought it might be good to encourage more "thinking out loud" in quantitative ways, even while you're still fleshing a model out and still have a lot of open questions about it)
Replies from: rocurley, Pablo_Stafforini, Pablo_Stafforini, Pablo_Stafforini, Lukas T, Lukas T, clearthis, Pablo_Stafforini, elityre, Pablo_Stafforini↑ comment by rocurley · 2020-03-09T02:25:13.439Z · LW(p) · GW(p)
Here's my bay area hospital capacity model: https://www.getguesstimate.com/models/15278
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-09T01:55:45.686Z · LW(p) · GW(p)
Here's a basic SIR model created by Metaculus user Isinlor. (I haven't looked at it, so don't interpret this comment as an endorsement.)
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-10T00:05:00.848Z · LW(p) · GW(p)
Buck's tentative Guesstimate model [LW(p) · GW(p)] of Wei Dai's "hospital crowding" catastrophic scenario. Many folks have already seen his comment, but I'm posting a link to it for completeness.
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-10T00:02:25.020Z · LW(p) · GW(p)
Daniel Filan's Guesstimate model [LW(p) · GW(p)] on whether he should stay home for work. Many folks have already seen his comment, but I'm posting a link to it for completeness.
↑ comment by Lukas Trötzmüller (Lukas T) · 2020-03-10T09:34:03.168Z · LW(p) · GW(p)
When to cancel events due to Coronavirus? Calculations by Linch Zhang [1], I've put them into a Guesstimate with some slight changes and adaptions for Austria [2]
[1] https://docs.google.com/document/d/1A0jcxj4n0BvNt_jMunHT5WSsAKFzuVJJyaaqcK9Z1HU/edit#
↑ comment by Lukas Trötzmüller (Lukas T) · 2020-03-10T09:31:35.354Z · LW(p) · GW(p)
Dating during Coronavirus: What's the risk of going on a date with a random new person at the height of an outbreak? https://www.getguesstimate.com/models/15381
Under my assumptions, if 1 in 7700 people gets newly infected every day, it translates to an infection risk of 0.2% per encounter (range of 0.45% - 0.053%). Feedback welcome.
↑ comment by Tobias H (clearthis) · 2020-03-09T18:04:02.898Z · LW(p) · GW(p)
Here's a tool to estimate how badly hospitals will be overfilled in your community.
It's by Richard Neher and colleagues and an early stage tool. Might nevertheless be interesting to play around with.
Here's the source and some explanations about the underlying model:
https://twitter.com/richardneher/status/1236980631789359104
Replies from: ErickBall↑ comment by ErickBall · 2020-03-09T21:21:59.290Z · LW(p) · GW(p)
Unfortunately it doesn't let you modify the assumptions about disease severity or number of undetected cases. It assumes that the majority of cases have been undetected (which seems questionable) and that 4.31% of cases are severe (which seems low even if the majority are undetected). It gives a case fatality rate of 0.97%, which doesn't seem to depend on any of the other parameters.
In their baseline scenario (for a small Swiss city with good infection control) 0.26% of the population dies.
With no infection control this goes up to 0.76% of the population dying, with no change in the CFR.
If you also increase the length of a hospital stay from 10 days to 20 days, the total number of deaths actually decreases slightly because the spread is slower. So while the graph is a nice way to see how long hospitals will be overwhelmed in different scenarios, it doesn't show you anything useful about how this affects outcomes. I would love to be able to add in some parameters for fatality rate for severe and critical cases with/without a hospital bed.
Replies from: cousin_it↑ comment by cousin_it · 2020-03-09T21:45:10.932Z · LW(p) · GW(p)
In their baseline scenario (for a small Swiss city with good infection control)
Sad laugh. I'm in Switzerland, we have exponential growth and there's no infection control to speak of. They just told people with non-severe symptoms to not bother getting tested. Schools are open. Haven't seen even one person wearing a mask.
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-11T14:53:48.934Z · LW(p) · GW(p)
Another basic SIR model, which considers impacts on hospital capacity (and resulting deaths) from infection controls of various degrees.
↑ comment by Pablo (Pablo_Stafforini) · 2020-03-09T13:37:35.782Z · LW(p) · GW(p)
The Medium article that Wei Dai cited in his comment [LW(p) · GW(p)] links to an "open-source model". I haven't examined it closely, though I did notice that some of the formulas are weirdly constructed (e.g. using INDIRECT rather than absolute cell references) and that some of the assumed parameters are overly pessimistic (e.g. a 3.4% CFR).
comment by Steven Byrnes (steve2152) · 2020-03-25T00:56:03.593Z · LW(p) · GW(p)
I'm still pondering the implications of transmission being mainly about air, not touching [LW · GW]. What interventions does that suggest? Besides the obvious things (opening windows [LW · GW], HVAC filters etc, masks & goggles), one thing I thought of is ... perfume!
We could all encourage everyone to wear perfume / cologne when they leave their home, and if anyone can smell anyone else, then they know you're not sufficiently well physically-distanced (too close or not enough air circulation).
Assuming this would work, I'm not sure how to get it to take off. Maybe an unusually considerate boss of an could tell their employees to all wear perfume (if they have any), to help ensure that everyone is keeping safe distance from each other, and to identify HVAC gaps? Or I could wear perfume and a hat / T-shirt that says "if you can smell my perfume, you're too close!" I dunno, just brainstorming :-P
comment by Wei Dai (Wei_Dai) · 2020-03-23T05:32:08.248Z · LW(p) · GW(p)
Suppose one of the drugs under investigation for COVID-19 effectively reduces its morbidity and mortality. For simplicity let's say that it quickly and completely cures 90% (or X%) of patients but does nothing to the remaining 10%, and we manage to scale up manufacturing enough to be able to treat everyone with the drug. Would the major developed countries then decide to relax the current mitigation/suppression policies and let the pandemic run its course (thereby accepting the morbidity/mortality of the refractory 10%) in order to revive their economies? What do you think the threshold for X would be for the major developed countries to do this?
Replies from: romeostevensit↑ comment by romeostevensit · 2020-03-23T09:21:29.332Z · LW(p) · GW(p)
I feel like there's wet spaghetti code at both ends of this? On one side we have economic impact projections that vary about an order of magnitude and the other we have expected death projections that vary over 1-2 orders of magnitude.
comment by madhatter · 2020-03-22T10:24:19.091Z · LW(p) · GW(p)
Someone on Hacker News had the idea of putting COVID patients on an airplane to increase air pressure (which is part of how ventilators work, due to Fick's law of diffusion).
Could this genuinely work?
Replies from: chris-hibbert-1↑ comment by Chris Hibbert (chris-hibbert-1) · 2020-03-22T19:00:47.966Z · LW(p) · GW(p)
Airplanes pressurize to levels that aren't as high pressure as being on the ground, I'm pretty sure. They're trying to reduce the consequences of being at altitude, not increase above sea level.
comment by DanielFilan · 2020-03-21T21:47:49.463Z · LW(p) · GW(p)
The New York Times heavily implies that many sick package delivery workers are feeling pressured to show up to work despite their illness.
comment by FactorialCode · 2020-03-20T05:13:11.074Z · LW(p) · GW(p)
A sneak peak at the coming economic impact:
Google trends: How to file for unemployment.
https://trends.google.com/trends/explore?date=today 3-m&geo=US&q=how to file unemployment
comment by Joel Chan (joel-chan) · 2020-03-20T03:04:35.959Z · LW(p) · GW(p)
Many have probably seen the threads (e.g., here and here, and this Medium post by Yishan Wong) about how massively scaled up testing is the key to threading the needle between economic collapse (long-term suppression tactics) and unacceptably high mortality (mitigation only, or worse, doing nothing). Aggressive and scaled up testing infrastructure is the key enabler for contact tracing, which appears to be the cornerstone of the South Korea model, which notably does not rely on draconian suppression tactics like lockdown, and they are currently the only other country than China (that I know of) that has R0 < 1.
I'm now wondering if, in the spirit of wartime efforts, more people can be trained to help power this testing infrastructure than can be trained to help increase our healthcare capacity.
comment by sprague · 2020-03-15T16:35:53.678Z · LW(p) · GW(p)
Is somebody keeping track of the "what if we're wrong and it turns out this is another Y2K" scenario? Social distancing, closing borders, heightened awareness and preventative measures -- seems like a lot is happening that could make this way less scary, at least in the US, than most of the mainstream scenarios.
I'm not interested in the hearing from denier-types who think this is "just another flu", but rather the thoughtful people who have specific testable predictions that would demonstrate this is more social contagion than most of us suspect.
Replies from: Vaniver, TobyBartels↑ comment by Vaniver · 2020-03-15T16:58:51.556Z · LW(p) · GW(p)
Is somebody keeping track of the "what if we're wrong and it turns out this is another Y2K" scenario?
That is, a combination of "prevention work successfully means no big disasters" and "absence of prevention work doesn't cause any major disasters"? I think that cat is already out of the bag on the latter one; people might end up disagreeing on whether it was better to be in Iran or Wuhan, but they won't be able to disagree that the lockdown in Wuhan had an effect.
I think there will be variation in what sorts of social distancing happen, which we should be able to back out data on, and similarly demonstrate that social distancing had an effect. (I expect it'll be smaller than many people hope it'll be, but it'll still be noticeable.) Like, we could see the effect in 1918 influenza data, and we have a much better ability now to track how people come into contact with each other.
[I expect the main thing to happen is that people take insufficient protective measures, which makes them look like a waste, or we get stuff like "ah look, extensive social distancing meant the peak happened two weeks later!", which is of unclear value compared to the costs.]
Replies from: sprague↑ comment by sprague · 2020-03-16T00:09:35.334Z · LW(p) · GW(p)
Those arguments make sense, but for example what if despite our best modeling, the cases just start to decline and then the whole thing just disappears in a month? At what point would we have to seriously re-evaluate everything we know about this virus? Say new cases plunge 90% next week? 50%?
Scenario planners try to think of every possible alternative, including those that seem far-fetched. I'm trying to figure out what the positive alternatives would look like.
Replies from: Vaniver↑ comment by Vaniver · 2020-03-16T02:10:31.110Z · LW(p) · GW(p)
From A Technical Explanation of Technical Explanation [LW · GW]:
How would I explain the event of my left arm being replaced by a blue tentacle? The answer is that I wouldn’t. It isn’t going to happen.
If a miracle happens, then a miracle happens. I'm not holding my breath.
The ways in which I do expect Vaniver_2021 to look back at Vaniver_2020 and think "yeah, he was worried about that but it didn't turn out to be relevant" are various unknowns about the virus that might be fine or might be bad. For example, we don't know how bad surface transmission will be, but that's a big factor in what sort of isolation protocols you need to have. We don't know whether existing anti-virals will be effective. We don't know how long immunity will last, but that's a big factor in whether or not 'herd immunity' strategies will work, and how valuable it is to not catch it. We don't know how big a deal antibody-dependent enhancement will be, or how that will interact with the duration of immunity. We don't know what long-term effects of infection (think fatigue, disability, infertility, etc.) look like. We don't know how long people are infectious before they show noticeable symptoms.
For all of those things, I put significant probability on the "it's fine" side of the uncertainty. But it being not fine is quite bad compared to it being fine, such that the expected utility shakes out that I should take it seriously until we know more. For example, I now think that if you're taking your temperature every day, the "infectious before noticeable symptoms" window is probably about a day, which seems pretty tolerable, but don't think I made a mistake in my assessment before. If the long-term disability risk turns out to be closer to 1% than 10%, then I'll adjust my prior on long-term disability for next time (in the obvious way that I'll have two datapoints instead of one), but I won't think "oh, I cried wolf."
↑ comment by TobyBartels · 2020-03-15T18:18:47.211Z · LW(p) · GW(p)
I thought that we were right about Y2K, people spent a lot of time preparing for it, and their hard work saved us all. Is that wrong? (I understand if you just link to somewhere else and don't clutter up your thread any further with this digression.)
Replies from: Vaniver, sprague↑ comment by Vaniver · 2020-03-16T02:12:50.862Z · LW(p) · GW(p)
According to some as summarized by wikipedia, there's not all that much evidence that people who didn't prepare were bitten by it, or that fixing ahead of time was cheaper / better than fix-on-failure.
↑ comment by sprague · 2020-03-15T23:59:28.707Z · LW(p) · GW(p)
I mean Y2K in the sense of lots of fretting about something that turns out not to happen, whether because of significant preparation or from just being wrong about the urgency.
I realize it doesn't seem likely, but in the spirit of humility before humanity's collective ignorance, how might we know we were wrong? Like, clearly nobody's expecting US cases to suddenly level off and then disappear, but what if that happens anyway? At what point would we say we were just totally wrong?
comment by ErickBall · 2020-03-12T23:42:04.248Z · LW(p) · GW(p)
Ohio health official estimates 100,000 people in state have coronavirus:
This sounds crazy, but I don't understand the methodology so I'm not sure... Do people think it's plausible?
Replies from: pktechgirl, ErickBall, gwillen, Davis_Kingsley, jacobjacob, lennard-iosif↑ comment by Elizabeth (pktechgirl) · 2020-03-13T00:19:57.000Z · LW(p) · GW(p)
I can't rule it out, but it doesn't sound like this estimate was arrived at through sound practice.
↑ comment by ErickBall · 2020-03-13T13:31:34.695Z · LW(p) · GW(p)
Follow-up: Trevor Bedford has also debunked the claim in this twitter thread, saying that by the time Wuhan had 100,000 infections there were 1000 severe cases and 300 deaths. For Ohio to be in that state now the disease would have had to be spreading there since about mid-December.
Replies from: michael-mclaren↑ comment by Michael McLaren (michael-mclaren) · 2020-03-14T08:07:17.537Z · LW(p) · GW(p)
This ^...Another way to spot check the "100000 cases" estimate without knowing the Wuhan numbers is to consider that that would imply roughly 1e5 / (2^4) = 6250 cases 3 weeks ago (the typical delay between infection and death; assuming 6 day doubling time), which corresponds to 31-125 deaths by today for a case fatality rate in the interval of [0.005, 0.02]. That would be for Ohio alone. As of March 13, the US CDC is only reporting 36 deaths for the country as a whole (source; though reported as 47 deaths here) and Ohio is currently reporting 0 deaths (source). Not to say that this is a definitive argument against there being 100000 cases in Ohio, but it does suggest that this estimate wasn't based on current understanding of the virus and its spread.
Update: On March 13 Trevor Bedford also tweeted a rough estimate of 10K-40K cases nationally.
↑ comment by Davis_Kingsley · 2020-03-13T05:13:08.389Z · LW(p) · GW(p)
I believe it's obviously wrong and the stated methodology makes no sense. The fact that community transmission is occurring does not by any means mean that 1% of the population is affected. It's possible there's some other information that justifies this but I would be *extremely* surprised if it were actually the case that 100k people are infected in Ohio right now.
↑ comment by Bird Concept (jacobjacob) · 2020-03-13T04:48:48.560Z · LW(p) · GW(p)
If this was the case it ought to be visible indirectly through its effect on Ohio's healthcare system. I haven't heard of such reports (and I do follow the situation fairly closely), but I haven't looked for them either.
↑ comment by Lennard Iosif (lennard-iosif) · 2020-03-13T04:59:59.457Z · LW(p) · GW(p)
Adding to this - what impact would this have on Wei Dai's estimates on mortality rates skyrocketing if health systems are overburdened? If significant portions of the population already have the illness, then would that imply a significantly lower mortality rate than expected? Or could this simply be a leading indicator that we are closer to the peak than we originally thought?
comment by AlexSchell · 2020-03-11T19:06:33.870Z · LW(p) · GW(p)
How should I disinfect objects with complex surfaces (e.g. box cutters, door knobs) if I don't have access to alcohol? Is brushing with soap likely to be sufficient or should one just avoid touching these objects for a few days if they're possibly contaminated?
Replies from: Original_Seeing↑ comment by Original_Seeing · 2020-03-12T18:04:29.285Z · LW(p) · GW(p)
https://www.journalofhospitalinfection.com/article/S0195-6701(20)30046-3/fulltext#sec3.1 lists a lot of different disinfectants.
3-4 is decent. 4+ is good.
Do you have any disinfectants at all?
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T18:21:48.241Z · LW(p) · GW(p)
Thanks! I didn't realize how effective bleach is. I recently moved and didn't get around to stocking up on any alcohol until it was out of stock in most places. I am expecting a shipment of industrial ethanol (still available, just don't ingest/get on your skin) but the bleach will arrive sooner. Thanks again.
Replies from: Original_Seeing↑ comment by Original_Seeing · 2020-03-13T17:27:55.295Z · LW(p) · GW(p)
Depends on what kind of bleach it is, but many chemicals commonly called bleaches are very strong. Hydrogen Peroxide is broad-spectrum and very effective.
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-13T20:34:31.209Z · LW(p) · GW(p)
I meant sodium hypochlorite
Replies from: jkaufman↑ comment by jefftk (jkaufman) · 2020-03-15T02:04:27.198Z · LW(p) · GW(p)
I wrote something looking into bleach: https://www.lesswrong.com/posts/QJfiKwicwTXYMzJ7q/bleach [LW · GW]
Summary: it's extremely concentrated, and a highly recommended disinfectant, but it's also dangerous and you need to be careful with it in specific ways
comment by rmoehn · 2020-03-09T21:25:15.997Z · LW(p) · GW(p)
How about an app that trains you not to touch your face?
Point your phone's camera or a webcam at yourself while you're working. The app produces a beep whenever you move your hand near your face.
Technically feasible, I'd say. Someone familiar with iOS/Android computer vision APIs should be able to put it together in a few days.
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2020-03-09T22:03:17.170Z · LW(p) · GW(p)
It exists.
Replies from: Raemon, rmoehncomment by Shmi (shminux) · 2020-03-09T00:13:21.827Z · LW(p) · GW(p)
I wish I didn't have to see the deluge of coronaposts in my feed or under Latest Posts.
Replies from: Benito, Raemon↑ comment by Ben Pace (Benito) · 2020-03-09T01:22:02.754Z · LW(p) · GW(p)
One of the reasons this thread exists is for that content to go here instead :)
comment by Alexei · 2020-03-19T20:29:49.330Z · LW(p) · GW(p)
My wife's doctor said chloroquine (a treatment for malaria) was shown to be very promising in treating COVID-19. I guess it's public now as well: https://www.wired.com/story/an-old-malaria-drug-may-fight-covid-19-and-silicon-valleys-into-it/
Replies from: zby↑ comment by zby · 2020-03-23T13:10:29.992Z · LW(p) · GW(p)
This is interesting subject - can we do here better than official science? As I understand the situation now there are still no good trials on this. There is one Italian trial that was heavily criticized: https://news.ycombinator.com/item?id=22662103 , and one Chinese that has not been published yet: http://www.chictr.org.cn/showprojen.aspx?proj=48880 - and some older ones for SARS https://www.ncbi.nlm.nih.gov/pubmed/15351731?dopt=Abstract
But maybe soon we'll have better data: https://www.sciencemag.org/news/2020/03/who-launches-global-megatrial-four-most-promising-coronavirus-treatments
I think official science should be pretty good on this one unless we find some mismatching incentives like in Inadequate Equilibria
comment by romeostevensit · 2020-03-19T01:42:03.331Z · LW(p) · GW(p)
Subway use in New York is only down 20%. And mask use is rare. How is NY not completely screwed?
Replies from: romeostevensit↑ comment by romeostevensit · 2020-03-20T09:25:22.787Z · LW(p) · GW(p)
He's still basically claiming over reaction but at least this is something major.
comment by DanielFilan · 2020-03-17T06:15:17.456Z · LW(p) · GW(p)
How much should COVID-19 update me about the risks from pandemics?
Replies from: Kaj_Sotala, ChristianKl↑ comment by Kaj_Sotala · 2020-03-17T09:52:31.199Z · LW(p) · GW(p)
That probably depends on what your pre-COVID-19 model was?
If I rephrase the question as "how much should COVID-19 update expert models about risks from pandemics", then my impression is that things have proceeded roughly in line with the pre-existing models. The response procedures that are now being activated in several countries are based on plans that were originally made as a reaction to previous diseases such as SARS.
My own update is that although there has been some feet-dragging, overall the national responses have felt stronger and faster than I would have anticipated. The next time that there is a pandemic, such a response should hopefully be more routine and competent, so this makes me more optimistic about our ability to deal with future pandemics.
↑ comment by ChristianKl · 2020-03-19T17:34:49.680Z · LW(p) · GW(p)
LessWrong censi did frequently list pandemics as concern for the annihilation of the human race for many participants. To me this episode suggests that as a group we were right to be more concerned then the average person on the street.
I would expect the crisis to increase public funding of pandemic intervention a lot, so the objective risk will go down in comparison towards pre-COVID-19.
I think it makes sense to go from the previous majority opinion that pandemics are the biggest x-risk to consider AI risk the biggest x-risk with pandemics at the second place.
Replies from: DanielFilan↑ comment by DanielFilan · 2020-03-19T18:19:26.377Z · LW(p) · GW(p)
Presumably COVID-19 should update me on natural pandemics happening more frequently than I would have otherwise thought though, right?
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-19T20:28:17.284Z · LW(p) · GW(p)
Of course it's Bayesian evidence for natural pandemics happening more frequently, but the size of the update depends on your previous model.
People who think that climate change is a more serious threat then pandemics should likely update towards pandemics being more serious but I don't think that includes most of our community.
There's a chance that calling this a natural pandemic in the way an earthquake or a supervulano eruption is natural is also misleading. There's a good chance that this pandemic was acciendently created by the human institution of a wild animal market in China. Xi's China seems authoritarian enough to shut down those markets in the future.
Our preparedness towards pandemics was really screwed up. This cricis will affect the public psychy like 9/11 and we will do a lot to get future safety.
comment by Ben Pace (Benito) · 2020-03-16T21:07:18.880Z · LW(p) · GW(p)
I thought I'd share the steps my housemates and I have taken to be safe from the coronavirus, just to spread info about what people are doing. I'd be interested in others saying some things that they've done. This isn't exhaustive, I've almost certainly forgotten some things. (Note that we live in Berkeley, California, US.)
- We don't meet anyone from outside the house / go to work / go shopping, and generally stay in the house/garden. Some housemates take walks / go for a run, keeping 6 feet away from people at all times.
- If anyone thinks there's a need to leave for any reason, even if it's to help the house in some way, they get permission either during a house meeting or via the house Slack.
- We've put up proper hand-washing signs by all the sinks, and all do this regularly including around mealtimes.
- We have stored about 3 months of food and necessities per person. Every 2 weeks, we'll order 2 weeks of food+necessities on Amazon/Instacart, to have a clear headway in case any ordering services end up having month-long delays due to massive rise in demand.
- We have bought a cheap car for any important travel and also to take trips to places where there are no people (to go for walks and so on).
- We've covered basically all doorhandles, edges of drawers, and similar surfaces, with copper tape.
- We leave packages outside for 2 days before opening them, or else using gloves, throw the cardboard away, disinfect the contents with disinfectant wipes, then remove gloves.
- I'm taking a multi-vitamin each morning for the vitamin D.
- Oli and I have set up an office space on the top floor outside my bedroom, with desks and monitors and such.
A few other our-situation-specific things we've done.
- One person recently came back from international travel, so we got them a small solo AirBnb for 10 days and provided them with lots of food and snacks, to confirm that they're symptom free. (They were careful on the flight, using disinfectant wipes on the plastic on their seat, not accepting anything from cabin crew, etc.) They'll return to the house this week.
- We had a non-rationalist renter who was moving out in the next month or so. They were unfortunately still using public transport and going to work, so we paid for them to have an AirBnb for that duration, and they've now finally moved out.
- I got a VR headset for fun and exercise (BeatSaber is great!).
There's a bunch more things we've done for the community, though that overlaps with things the LW team has done (e.g. Ray set up a community-wide spreadsheet for people to report the steps they'd taken and what level of exposure they are at).
comment by K2msmith · 2020-03-15T06:27:19.859Z · LW(p) · GW(p)
Write or message your local county public health department to include a history of the number of new cases per day not just the current total on their covid-19 website. Growth rate is just as important as the current state.
Replies from: chris-hibbert-1↑ comment by Chris Hibbert (chris-hibbert-1) · 2020-03-22T18:59:14.269Z · LW(p) · GW(p)
I've been following the daily numbers from California, Washington state, and New York, on covid2019.app, which were extremely informative, but they stopped reporting by state as of two days ago. Anyone know of a good source for daily state level new case data?
Summary: CA, WA, and NY had all reached 100 reported daily new cases by 3/14. Up to 3/19, neither CA, nor WA had broken through 200 new cases, but on 3/18, NY reported 1709 new cases, and on 3/19 they had 1069. The state level data is not available at the moment (when the site was working better, it said state level would be available), and even the regional data is broken in the current download.
Replies from: PeterMcCluskey↑ comment by PeterMcCluskey · 2020-03-22T22:11:34.774Z · LW(p) · GW(p)
I use https://en.wikipedia.org/wiki/Template:2019–20_coronavirus_pandemic_data/United_States_medical_cases
Replies from: chris-hibbert-1↑ comment by Chris Hibbert (chris-hibbert-1) · 2020-03-25T16:23:40.468Z · LW(p) · GW(p)
Thanks, Peter! very helpful.
Update on the data: NY is now adding 5000 new cases per day. WA is above 200, and CA above 250. No one looks like they're stopped the growth in new cases. A slow exponential is still exponential.
Replies from: Unnamed↑ comment by Unnamed · 2020-03-25T22:34:30.279Z · LW(p) · GW(p)
Keep in mind that the trend in the number of confirmed cases only provides hints about the trend in new infections. The number of confirmed cases is highly dependent on the amount of testing, and increases in testing capacity will tend to lead to more confirmed cases. Also, there is a substantial delay between when a person is infected and when they test positive, typically somewhere in the range of 1-2 weeks (with the length of the delay also depending on the testing regime).
comment by DanielFilan · 2020-03-14T05:05:48.306Z · LW(p) · GW(p)
Anybody know the rough cost-benefit tradeoff of donating blood products a doubling or two from now? [EDIT: this place is not packed, but there are people there, and I'm obviously in contact with the nurses]
Replies from: chris-hibbert-1↑ comment by Chris Hibbert (chris-hibbert-1) · 2020-03-22T18:32:24.008Z · LW(p) · GW(p)
The donor centers are probably the cleanest place you can visit outside an ICU. Their standard hygiene practices are superb and have been so since the HIV epidemic decades ago. (I've been giving blood routinely for at least 35 years.) Even if someone were to visit who had been exposed, there's little chance they could transfer it to anything that would transfer it to you. The one opportunity you have to be close to other people who aren't being extremely cautious at all times is in the canteen for your mandatory 20 minute break after donating, and unless the donor center is extremely crowded, you'll be able to maintain a 6 foot separation and not touch anything that isn't freshly removed from packaging for your use.
I donated platelets a week ago. I stopped donating whole blood ~ a year ago after noticing that it impacted my ability to exercise (blood oxygenation, presumably) for a few weeks after donating. Now that I'm sheltering-in-place and not getting any of my usual aerobic exercise, I'm considering giving whole blood once I've passed the waiting period.
comment by Alexander Mont (alexander-mont) · 2020-03-12T23:22:01.321Z · LW(p) · GW(p)
I'm currently in an apartment in Washington, DC living with one other family member. I have decided that I want to self-quarantine completely (i.e. no leaving the apartment, deliveries only), and the other person is saying that they are willing to mostly quarantine (i.e. work from home, no trips to the store, etc.) but they aren't willing to refuse to go outside.- they want some fresh air. Is there a good way of modeling the risk associated with just going outside and walking around? And of the family member then giving it to me? I do have another place to go all by myself but I would rather be with my family and I'm trying to get a sense of what the additional risk is.
I'm 32 years old and most concerned with the idea that I will get infected and the hospitals will be filled up so I won't be able to get a spot. I almost think that the safest place to be right now is somewhere like Hong Kong, South Korea, or Singapore, that's already contained their outbreak? Should I just get on a plane right now to one of those places? (I can easily afford the ticket)
Replies from: habryka4, chris-hibbert-1↑ comment by habryka (habryka4) · 2020-03-12T21:58:24.136Z · LW(p) · GW(p)
At our group house we decided that going out on walks is fine, as long as you stay more than 6-feet away from people. I am not sure whether that's feasible where you are, where we are it's feasible, but only at times of the day that tend to have less people around.
Replies from: Raemon↑ comment by Chris Hibbert (chris-hibbert-1) · 2020-03-22T18:37:25.306Z · LW(p) · GW(p)
Going outside for solo exercise (walking, jogging, Tai Chi) is pretty safe. I'm not absolutely positive that tennis or volleyball (multi-player sports, but with shared contact with the ball) or ultimate frisbee or basketball (close proximity, occasional contact) are as safe. The SF Bay area shelter in place order encouraged going on walks or hiking, and that seems sensible to me.
comment by Unnamed · 2020-03-12T21:59:42.730Z · LW(p) · GW(p)
Here's a method to try to estimate the number of cases in a region which I haven't seen calculations of:
1. Identify the places which have the best testing regimes
2. Try to estimate what fraction of cases are identified in those places, potentially along with other variables like how long from infection until the case is identified
3. Use those numbers to extrapolate to other places, based on other similarities between those places besides # of confirmed cases (e.g., number of deaths, or rate of infection in travelers coming from that place, or hospital utilization rate)
I have made some initially attempts to do this, which I'll try to post later today. I'm wondering if anyone has thoughts or sources on any of these 3 points (e.g., which places have the best testing regimes?), or on the method as a whole.
Replies from: Unnamed↑ comment by Unnamed · 2020-03-16T02:29:44.752Z · LW(p) · GW(p)
This paper looks at cases which were confirmed in Shenzhen (Guangdong, China) Jan 14 - Feb 12, which is while coronavirus was being brought under control there (by the end of the study the cases had fallen to less than 1/3 of their peak). I suspect that they qualify for point 1, a place with an unusually good testing regime.
The paper reports that "Cases detected through symptom-based surveillance were confirmed on average 5.5 days (95% CI 5.0, 5.9) after symptom onset (Figure 3, Table S2); compared to 3.2 days (95% CI 2.6,3.7) in those detected by contact-based surveillance", and also that the median incubation period was 4.8 days from infection to symptom onset (in the smaller sample where both of those dates were known).
Adding 5.5+4.8, that implies that an average of 10.3 days passed between when a person became infected and when they tested positive for cases detected based on symptoms, and 8.0 days for those detected by contact tracing. Since the paper reports that 77% of cases were detected through symptom-based surveillance, that gives an overall average of 9.8 days. (And this is only for the cases that were detected; it's not adjusting at all for people who were infected by never got a positive test.)
That means that in places where testing is as good as it was in Shenzhen, then the number of positive tests is telling us about the number of infections 9.8 days ago. If the number of cases in that region is doubling every 4 days, then that's 2.4 doublings, so the number of confirmed cases would only be 18% of the actual number of cases due to the delay in testing (again, without factoring in people who never got tested). (With a 3 day doubling period it would be 10%, with a 5 day doubling period 26%.)
So in places that don't have a good testing regime it would be significantly less than that.
comment by Sherrinford · 2020-03-12T20:37:33.090Z · LW(p) · GW(p)
Here is a summary of an ebook about the economics of the Coronavirus:
http://conversableeconomist.blogspot.com/2020/03/some-coronavirus-economics.html
It also contains this figure:
{kind=link}
comment by ChristianKl · 2020-03-10T18:32:15.233Z · LW(p) · GW(p)
I have the impression that there are a lot of windows in public transportation that currently aren't opened due to it being cold outside.
It's likely beneficial to get to a state where all the windows in public transportation that can be opened are actually opened.
There might be a high value in pushing that meme as it's an easy intervention.
comment by vidro3 · 2020-03-09T06:09:42.779Z · LW(p) · GW(p)
Is it anticipated that COVID-19 will have more estimated cases than the seasonal flu? Would appreciate a link to supporting info.
Is R0 the best way of measuring contagiousness?
Replies from: justin_dan, pktechgirl↑ comment by justin_dan · 2020-03-10T03:45:15.589Z · LW(p) · GW(p)
Someone on Reddit linked to this preprint paper arguing that the other moments of the secondary infection curve (variance, skewness, kurtosis) can overwhelm the mean (i.e., the R0) in predicting the number of people ultimately infected. With a high variance, right-skewed, high kurtosis curve (loosely, with relatively few "super-infectors" bringing up the average), there are more chances for the outbreak to stochastically die out before those super-infectors get their chance to keep things going. The authors conclude that "higher moments of the distribution of secondary cases can lead a disease with a lower R0 to more easily invade a population and to reach a larger final outbreak size than a disease with a higher R0. " I'm not positioned to evaluate all of their arguments, but their reasoning based on the models they provided made sense as far as I could tell, using some assumptions that seemed fairly reasonable to this layperson.
The practical consequence of this is that effective contact tracing in the early stages of an outbreak (before too many so-called "community spread" cases) would provide invaluable epidemiological data.
Replies from: vidro3↑ comment by vidro3 · 2020-03-10T11:58:37.238Z · LW(p) · GW(p)
honestly have no idea what that all means. thanks for trying though.
Replies from: justin_dan↑ comment by justin_dan · 2020-03-10T16:16:16.688Z · LW(p) · GW(p)
R0 tells you how many others each person infects on average. So R0 is in one sense the measure of contagiousness--it just tells you how contagious people with the disease are on average.
Consider two different diseases with the same R0, let's say R0 = 2. So each person on average infects 2 others. For the first disease, almost all patients infect exactly two others, but for the second, plenty infect two, many infect one, and a much smaller number infect 10 or even more others. So the average is the same, but the distribution is very different.
Given some other assumptions, this paper shows that diseases more like disease one will end up infecting many more people in the end than diseases like disease two, even though they have the same R0. So it is important to understand the distribution of secondary infections in addition to the average when predicting the final outbreak size. Contact tracing (seeing who people with the disease came in contact with and checking to see whether they end up getting infected) allows epidemiologists to do that.
↑ comment by Elizabeth (pktechgirl) · 2020-03-09T05:08:50.994Z · LW(p) · GW(p)
R0 is not a great way of measuring contagiousness. For example, Ebola has an R0 of 1.5-2, and Influenza 1.1, but obviously many more people catch Influenza than Ebola.
I don't know if this is the cause of the problem with these particular numbers, but in general, R0 is very much a compound function of disease and environment, and therefor doesn't tell you much about how contagious something will be if you change behavior.
comment by jmh · 2020-03-26T13:17:06.481Z · LW(p) · GW(p)
Two related "wild" ideas, as I think we probably have the basic technology and knowledge but probably not something we can quite do now.
My understanding is that the virus is attacking the ACE2 molecules. These actually form a gateway between the interior of the cell and the external environment.
If so, in theory, we might be able to create a number of artificial "bodies" -- thinking just a lipid bilayer sack with some ACE2 elements attached. Any virus that binds with that will "infect" the dummy cell but have no way of replicating so effectively die and not infect the body.
Similarly, a mask, even one that is not quite as fine filtered as others, which is impregnated with such compounds might prove effective as a filter for this specific virus.
Anyone know of any virological sources that are might be digestible by non-experts that might discuss such approaches?
Replies from: leggi↑ comment by leggi · 2020-03-26T16:18:51.982Z · LW(p) · GW(p)
virus is attacking the ACE2 molecules.
This is very interesting information. I was wondering (but not enough to actually research it) why diabetes mellitus (DM) was a bigger risk factor of severe disease than I would have associated with the "normal" increased risk with infections in patients with DM.
A quick search led me to this article in the Lancet.
The expression of ACE2 is substantially increased in patients with type 1 or type 2 diabetes, who are treated with ACE inhibitors and angiotensin II type-I receptor blockers (ARBs).
Hypertension is also treated with ACE inhibitors and ARBs, which results in an upregulation of ACE2.
ACE2 can also be increased by thiazolidinediones and ibuprofen.
ACE2
(has a) functional receptor for the spike glycoprotein of the human coronavirus HCoV-NL63 and the human severe acute respiratory syndrome coronaviruses, SARS-CoV and SARS-CoV-2 (COVID-19 virus)Replies from: jmh
↑ comment by jmh · 2020-03-26T19:57:36.002Z · LW(p) · GW(p)
I believe there was also an issue related to glucose levels as well, which then results in worse infection outcomes with this virus.
I just came across the following that might be of interest as well: https://www.eurekalert.org/pub_releases/2020-02/msa-arc022620.php
That was from late February and I've not seen anything providing any update on the trials they were starting.
Not sure if that is working as I was thinking, a decoy to get the virus to bind with something other then the cell and so neutralizing it.
comment by streawkceur · 2020-03-25T13:42:09.668Z · LW(p) · GW(p)
Are there statistics/tables listing not only infections, but also not-infections with circumstances (X was quarantined because of contact with Y, but turned out to be negative)? This might help to assess the risk associated with certain situations (quickly buying something in a store, conversation in open air with distance, in a closed room etc.)
comment by AlexSchell · 2020-03-24T11:53:54.709Z · LW(p) · GW(p)
This looks sketchy to say the least (e.g all citations are self citations), but seems worth doing a very shallow dive into or pointing out if clearly flawed: claim that yogurt can prevent secondary bacterial pneumonia in COVID-19 patients. The argument seems to at least imply that secondary bacterial pneumonia leading to cytokine storm is a common pathway to fatal cases.
(H/t Rob Wiblin on Twitter)
Replies from: leggi↑ comment by leggi · 2020-03-24T13:18:36.572Z · LW(p) · GW(p)
Some quick thoughts if anyone wants to do a dive:
The article is talking about "live" yoghurt i.e. cultured milk with no other additives.
The main bacteria to culture milk into yogurt are:
Lactobacillus bulgaricus (Lactobacillus delbrueckii subsp. bulgaricus) and Streptococcus thermophilus.
In what countries do people eat a lot of natural live yoghurt? (per capita not overall amounts). Bulgaria (a clue in the name of the first bacterium) Russia? Greece? Spring to mind. Local knowledge would help here.
What are the demographics of those populations? (total population, % of old folks most likely to suffer severe disease)
What's the COVID19 situation in these places?
The link says:
The cytokine storm is induced by the virus and the bacteria acting together.
I would want to see some evidence for this statement for instance levels of secondary infections being tested/confirmed/reported. (and the use of antibiotics as prophylactic or therapeutic agents - could antibiotics making things worse in some cases by killing of the good bacteria too????
comment by Iwein · 2020-03-21T00:58:10.030Z · LW(p) · GW(p)
Is there any information on how exactly the testing process works? I'm trying to determine whether pool testing could be worthwhile. Test 10 samples at the same time to confirm if they're all negative. If not, test them all separately. At worst that's 11 tests to confirm postivie cases for 10 people, yet only one to clear 10. There's a million variables like expected infection saturation, grouping by symptoms/likelihood of infection, cost of the tests, duration of testing, number of test stations(is this even a bottle neck that needs a solution?) and of course there are better ways to group samples, but I'm no mathematician to think of a proper protocol/algorithm for that: group size of 100 with halving of the groups in case they test positive? To speed up the process the multiple samples needed for several stages of testing would be collected at the same time.
comment by micpie · 2020-03-17T20:09:24.410Z · LW(p) · GW(p)
Interesting comment on a (maybe) new symptom, i.e., loss of smell and taste for several days, of a COVID-19 infection in an interview of a MD with focus on Virology in Germany:
Google translation of the interesting part:
"Almost all infected people we interviewed, and this applies to a good two thirds, described a loss of smell and taste lasting several days. It goes so far that a mother could not smell the full diaper of her child. Others could no longer smell their shampoo, and food began to taste bland. We cannot yet tell exactly when these symptoms will appear, but we believe a little later in the infection." (emphasize mine)
Sample size: approx. 100 patients, not very severe cases, i.e., no hospitalization (stated in the interview).
German newspaper source: https://www.faz.net/aktuell/gesellschaft/gesundheit/coronavirus/virologe-hendrik-streeck-ueber-corona-neue-symptome-entdeckt-16681450.html
Google translate link to English: https://translate.google.com/translate?hl=en&sl=de&u=https://www.faz.net/aktuell/gesellschaft/gesundheit/coronavirus/virologe-hendrik-streeck-ueber-corona-neue-symptome-entdeckt-16681450.html
However, I am not sure what the base rate of smell and taste loss is during an influenza or common cold infection?
comment by Richard Meadows (richard-meadows-1) · 2020-03-17T19:31:55.437Z · LW(p) · GW(p)
I am suspicious of the general advice against non-frontline health workers using masks (i.e. that anything short of a properly-fitted N95 mask is not only useless, but possibly does more harm than good). This air filter company claims that not only are masks a lot better than nothing; even home-made masks bodged out of cotton t-shirts or pillowcases catch 50-60% of virus-sized particles. Or as Naval suggested on Twitter, "billions of Asians aren't wrong."
I don't know whether this is correct, but am leaning towards wearing a mask in public (I have a cloth cycling mask with insertable filters, so I'm not keeping them from medical professionals). Has anyone looked into this?
Replies from: Raemon↑ comment by Raemon · 2020-03-17T19:43:20.172Z · LW(p) · GW(p)
See previous discussion here:
https://www.lesswrong.com/posts/7K8fSFTnpfN4EBuZ8/how-useful-are-masks-during-an-epidemic [LW · GW]
↑ comment by Richard Meadows (richard-meadows-1) · 2020-03-18T19:55:02.380Z · LW(p) · GW(p)
Cool, thanks. Still seems v. inconclusive... if anyone has more info, please chime in on that thread!
comment by streawkceur · 2020-03-16T23:39:34.025Z · LW(p) · GW(p)
Are there attempts to build an app that tracks everyone by GPS, and notifies all possible contacts (and people having been in the same supermarket etc.) when someone develops a cough?
It seems to me that, with a majority of people using such an app, the R0 could easily be pushed below 1 without too many restrictions. I think this could even work when using the app is on a voluntary basis - I guess that people making wrong statements in such an app and getting someone sick amounts to negligent assault in many countries.
I don't believe the claims that 60% of people getting infected - or even a month-long quarantine for everyone - is unavoidable with such a technology, and would like to hear differing opinions/see data suggesting the opposite.
Replies from: gwillen↑ comment by gwillen · 2020-03-16T22:31:48.494Z · LW(p) · GW(p)
There are at least two attempts I'm aware of to do almost exactly this, surely more that I'm not aware of, plus some attempts to do other modeling (like, using people's tracks from fitness apps, so they don't have to install a new app.)
I think it's going to be really unlikely to get enough people to use something like this to be useful, but I'd love to be wrong. If you want to help I'm happy to direct you to them.
Replies from: streawkceur↑ comment by streawkceur · 2020-03-17T21:56:38.391Z · LW(p) · GW(p)
I actually think it is plausible that governments and/or Facebook do this, and it becomes widely enough adopted.
A community-level risk score would already be helpful ("based on estimates in your locality, the risk of contracting the virus when taking a bus is X now...) for individuals.
Replies from: gwillencomment by jp · 2020-03-14T20:35:28.763Z · LW(p) · GW(p)
Does anyone want to venture a guess for the true number of cases in the Bay Area right now?
I just some rough back-of-the-envelope calculations, following the method here. Currently there are 2 deaths in the Bay Area. I keep his time-till-death rate of 17.3 days, but substitute a doubling time of 3 days, based on Our World in Data's US number. I get 2*100*exp(17.3*.231) ≈ 11,000, or about 2/1000 bay area residents. Super non-robust number, take with several grains of salt.
(.231 is the rate I get when solving for r in the exponential growth function for a doubling in 3 days.)
Replies from: kdbscott↑ comment by kdbscott · 2020-03-14T22:29:16.393Z · LW(p) · GW(p)
I've been a bit confused about doubling rate. First, I noticed that many numbers (e.g. Wikipedia) are calculating how long it took to double, instead of projecting forward using e.g. yesterday's increase. Early on this led to misleading numbers, but recently the US has been steady around 2-3 days using both methods.
However, I'm guessing that raw doubling rates depend a lot on testing, and that the US should expect to have a faster-than-actual doubling rate until our testing catches up. So I lean towards Trevor's number of 5 days.
comment by mako yass (MakoYass) · 2020-03-14T00:51:12.720Z · LW(p) · GW(p)
It had not occurred to me that there were any obvious companies a person could invest in to benefit from (and contribute to and accelerate) the response to the pandemic, but https://www.lesswrong.com/posts/yuyvosHTgjDR4giPZ/why-don-t-singularitarians-bet-on-the-creation-of-agi-by [LW · GW] mentions the videoconferencing software Zoom. It does seem to be the best videoconferencing software, from what I've heard. It's rare that I've ever had an international internet call from new zealand as stable as the ones I had on Zoom.
Any other industries a person could invest in? Food delivery, perhaps? In NZ I've been seeing lots of posters and qr codes in restaurants for a chinese service called Gogo, though if it's based in china we probably can't buy any of it.
comment by Alexander Mont (alexander-mont) · 2020-03-13T22:35:52.335Z · LW(p) · GW(p)
Hi, I have another few questions I'm interested in to help understand my own risks from the virus:
- What's a good estimate for the percentage of the US population infected, right now?
- What is the likelihood of transmission inside the home (i.e. if one of my family members gets it, what's the chance that I will get it?) What things can we do in the household to reduce this probability?
- I'm concerned about the possibility that if I get it, there won't be hospital beds available. Would it make sense to, at the first sign of symptoms, get on a plane to somewhere like Hong Kong or Singapore (or maybe Canada if things are better there) where things are more under control? That way there will be beds available if I need them. (Or maybe even do that preemptively, now?) Is that idea just totally crazy? (Money is no object)
↑ comment by Ben Pace (Benito) · 2020-03-13T22:54:03.704Z · LW(p) · GW(p)
What is the likelihood of transmission inside the home
My current working assumption is that if you share a living space and/or a bathroom with someone who gets it, you will get it within a few days. If you want to reduce the probability, make sure you don't use any common spaces or bathrooms.
comment by Original_Seeing · 2020-03-12T17:36:44.972Z · LW(p) · GW(p)
A strong preventative measure I haven't been hearing people talk about in general is constant cleaning of commonly touched surfaces. In workplaces and homes, this may be more valuable than encouraging people to wash their hands very often.
The Coronavirus can persist on steel, metal, wood, and plastic for up to 4 days according to the link below. Cleaning surfaces several times per day with an appropriate cleaning agent would therefore be highly valuable to implement.
There's not much point in constantly washing your hands if your office/home's front doorknob is spreading the virus to every person who touches it for 4 days in a row.
The SARS-CoVStrain P9 and HCOV listings in the link below are (I think) the best examples to look at. Best cleaning agents are those with 4+ "Reduction of viral infectivity (log10)" on the 2nd table.
https://www.journalofhospitalinfection.com/article/S0195-6701(20)30046-3/fulltext#sec3.1
comment by Eli Tyre (elityre) · 2020-03-11T23:18:38.986Z · LW(p) · GW(p)
Can we estimate what level of the disease will overtax US hospitals?
This page says that three are 924,107 "Total Staffed Beds in All U.S. Hospitals." Is that a good estimate of overall hospital capacity?
Does that mean that if/when ~ 1,000,000 people in the US have symptomatic cases, the hospital system will be at capacity?
Replies from: michael-mclaren, michael-mclaren, mark-xu↑ comment by Michael McLaren (michael-mclaren) · 2020-03-14T00:13:38.228Z · LW(p) · GW(p)
Comments on hospital capacity models from other threads in this post:
- https://www.lesswrong.com/posts/ACyGvQchWzGjGkKgS/coronavirus-open-thread#GXpQihDMgRA7EfgYS [LW(p) · GW(p)]
- https://www.lesswrong.com/posts/ACyGvQchWzGjGkKgS/coronavirus-open-thread#jC7CGd7KuuwLu5FT5 [LW(p) · GW(p)]
- https://www.lesswrong.com/posts/ACyGvQchWzGjGkKgS/coronavirus-open-thread#mYxKedFDALDS8v2S8 [LW(p) · GW(p)]
Other models / estimates:
↑ comment by Michael McLaren (michael-mclaren) · 2020-03-13T23:46:47.323Z · LW(p) · GW(p)
This preprint from Marc Lipsitch and colleagues is relevant,
Li R, Rivers C, Tan Q, Murray MB, Toner E, Lipsitch M. 2020. The Demand for Inpatient and ICU Beds for COVID-19 in the US: Lessons From Chinese Cities. https://dash.harvard.edu/handle/1/42599304
See their Figure 1 where they plot the hospitalization rate during the Wuhan epidemic against US hospital bed capacity to give an idea of how quickly the US would be overloaded in a "Wuhan-like outbreak". They consider ICU beds (2.8 per 10000 adults), empty ICU beds (31.8% of all ICU beds), and what they call "US inpatient beds in community hospitals" (29.7 per 10000 adults). The sum of ICU and community beds comes out to ~850000 based on an adult US population of 240 million, which isn't too far off from your 924107 number.
Two things to keep in mind for working through your question about the implications of 10^6 (concurrent) cases (I see these are reiterating points Mark already made): On the one hand, most symptomatic cases will not need hospitalization. On the other hand, most hospital beds are occupied (~70% of ICU beds, which roughly agrees with Mark's 66% estimate for overall beds), so the number of available beds is much less than the total number of staffed beds.
I've heard it suggested that today's declared national state of emergency and associated funding may enable things like FEMA building field hospitals to extend hospital bed capacity.
Edit: see also this blog post by author Eric Toner about the above preprint, http://www.centerforhealthsecurity.org/cbn/2020/cbnreport-03132020.html
↑ comment by Mark Xu (mark-xu) · 2020-03-12T08:20:49.708Z · LW(p) · GW(p)
Based on googling "hospital occupancy rates", about 66% of beds are already in use on any given day. Doctors I've talked to have said that extremely busy days result in near or over 100% capacity.
I expect that there is going to be gradual overload as COVID spreads through various communities, e.g. we're starting to see Washington hospitals starting to be overloaded
A rough estimate: there are ~333k empty hospital beds, a doubling time of 4 days, 300 new cases today, 0.2 percent of patients hospitalized and 14 days per hospitalization. Thus we want to solve for k such that , giving k > 34, so hospitals will be overloaded in 34 days. This estimate assumes that patients are distributed uniformly throughout all hospitals, so it's more of an upper bound given unchecked exponential growth.
Edit: Rob Wiblin provides an estimate (on FB) of 15k new cases in the US every day, giving k > 11.5. I haven't thought much about 15k new cases, but it seems far more correct than 300.
comment by Josh Jacobson (joshjacobson) · 2020-03-11T22:52:31.771Z · LW(p) · GW(p)
It seems plausible to me that the copper tape approach many LWers have adopted is counter-productive in at least some cases. The logic for this is:
1. In the pictures I've seen, and with my own applications of copper tape, to the surfaces we seem to touch most often (e.g. doorknobs, light switches) applications of it have created a number of small creases, bumps, ridges, and/or folds.
2. Copper does not seem to have nearly as strong an effect on surfaces as does wiping them with disinfectant.
3. Wiping them with disinfectant seems likely to be a lot less effective on surfaces that aren't smooth (bumps, ridges, etc.) due to the difficulty in wiping all parts of the surface.
Thoughts?
Replies from: gwillen, habryka4, Original_Seeing↑ comment by gwillen · 2020-03-11T23:47:59.288Z · LW(p) · GW(p)
I think the problem with this is the burden of wiping down surfaces often enough to be effective. Copper appears to take a few hours to effectively render the virus undetectable (according to https://www.statnews.com/2020/03/09/people-shed-high-levels-of-coronavirus-study-finds-but-most-are-likely-not-infectious-after-recovery-begins/, just out today.) So to get the same effect from wipes, I would presumably need to fully wipe down all those surfaces every few hours at least, and I would need to not run out of wipes.
I think for high-touch surfaces in widely-shared environments (e.g. offices), probably disinfecting every few hours or more often is a good idea, and better than the passive benefits of copper. At home I think copper is likely to win out, unless your house is really on the ball about disinfecting things.
↑ comment by habryka (habryka4) · 2020-03-11T22:56:48.556Z · LW(p) · GW(p)
I've also considered this. I think there is some chance of this being the case, and I think we should take it seriously. I've been considering sanding down all of the surfaces we covered with copper tape with sandpaper, to make sure they are actually smooth.
I do disagree with this though:
3. Wiping them with disinfectant seems likely to be a lot less effective on surfaces that aren't smooth (bumps, ridges, etc.) due to the difficulty in wiping all parts of the surface.
My current sense is that wiping them down with disinfectant works totally fine, since at least the disinfectant we use is pretty wet and seems to get into creases and bumps just fine.
↑ comment by Original_Seeing · 2020-03-12T17:58:31.690Z · LW(p) · GW(p)
A downside of using copper may be that exposing it to disinfectants could lead to a decrease in its efficacy. Ethanol is listed specifically.
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3067274/#r1
The claimed exception to this is "a 1% nonionic detergent solution".
comment by Sherrinford · 2020-03-11T22:21:34.351Z · LW(p) · GW(p)
My impression is that some Fermi estimate approaches assume that exponential growth indeed goes on until it hits the wall of 100%. Exponential growth is represented by ds/s = x, where s is the stock (here of infected people) and x is a constant. To my intuition, logistic growth ds/s = y (1-s) is almost as simple and it has the feature of a built-in limit. Of course both models imply 100% infection rates, but the second one asymptotically. The logistic model in this specification has highest absolute growth when 50% are infected, then lower (but still positive) growth because, e.g., infected people meet more who already infected.
Sorry if this is already common knowledge.
comment by Gurkenglas · 2020-03-11T15:38:58.797Z · LW(p) · GW(p)
Should we be buying something like oxygen concentrator/medical ventilator futures? This might make money and increase production. I'm not sure how to go about it, though.
comment by Ivan Denker (ivan-denker) · 2020-03-10T19:16:53.626Z · LW(p) · GW(p)
Assuming kids catch and spread the virus without sickening much, and that immunity among previously ill adults is robust, I would send my kids to a summer camp with immune counselors and lots of spit swapping (bobbing for apples, spin the bottle, being kids).
Any plausible way to use the mildness of illness in kids to develop herd immunity more quickly, rather than having them return home to parents and grandparents every day with deadly sniffles from the viral reservoir that is school?
Replies from: TobyBartels↑ comment by TobyBartels · 2020-03-15T18:32:10.119Z · LW(p) · GW(p)
Everybody says that immunity to coronaviruses is not robust (although we don't know yet about this specific one).
comment by Adam Zerner (adamzerner) · 2020-03-28T06:36:43.621Z · LW(p) · GW(p)
Is it possible that there are different viruses we're dealing with here? It just doesn't make sense to me that we're seeing such varying death rates, eg. Italy vs South Korea. The difference in medical quality doesn't seem like it can explain it.
Replies from: pktechgirl, leggi↑ comment by Elizabeth (pktechgirl) · 2020-03-28T14:10:24.876Z · LW(p) · GW(p)
There are already different strains identified, seems plausible some are worse than others.
↑ comment by leggi · 2020-03-28T07:34:28.960Z · LW(p) · GW(p)
The current tests are looking for the presence of a specific virus - looking at the genome using RT-PCR technology so the answer is no. (eek at being so definite)
PCR (polymerase chain reaction) is a DNA amplification technique
but Coronavirus is RNA so reverse-transcriptase (RT) is used to make a DNA 'template' from the RNA.
Some info. from Cambridge and Glasgow Universities regarding Covid-19 Genomics UK Consortium - A project to map how COVID-19 spreads and behaves by using whole genome sequencing will show if the virus is mutating.
Consider the demographics of the populations. Age, concurrent disease, levels of smoking, air pollution etc...
Levels of testing/recording/reporting....
(hope this makes some sense - written in a rush)
comment by Alexei · 2020-03-18T17:44:16.476Z · LW(p) · GW(p)
A random thought: If the virus doesn't survive well in high temperatures would going to a sauna help treat it?
Replies from: Vaniver↑ comment by Vaniver · 2020-03-18T17:48:31.182Z · LW(p) · GW(p)
This abstract says "Sauna takers should avoid bathing during acute respiratory infections." I haven't read the paper to figure out why they think that.
Replies from: Alexei↑ comment by Alexei · 2020-03-19T02:56:58.602Z · LW(p) · GW(p)
The whole abstract:
For over a hundred years Finnish sauna has been documented as a physiotherapeutic method in respiratory diseases. Physiological changes of ventilation remain small (about 10%) in the sauna. Heat load, sauna air and sympathetic stimulation generally do not cause problems to the lungs. Electron microscopic studies have not shown irreversible damages to the airway epithelium. Sauna takers should avoid bathing during acute respiratory infections. Sympathomimetic drugs may provoke tachycardia and arrhythmias in the sauna.
So I think they're specifically talking about bathing; while the sauna (dry air) is actually good.
I can't find the entire paper but if someone send me a link, I'll look more into it.
comment by willbradshaw · 2020-03-17T09:49:02.593Z · LW(p) · GW(p)
Last month, NIAID RML released an album of SEM and TEM images of SARS-CoV-2. This includes the multi-coloured image everybody is using but also a lot of other very striking images. Check it out!
comment by James_Miller · 2020-03-16T16:47:47.670Z · LW(p) · GW(p)
Consider getting a humidifier in case someone in your household gets COVID-19, because high humidity might reduce the transmission of the virus.
comment by Vanessa Kosoy (vanessa-kosoy) · 2020-03-16T15:02:52.925Z · LW(p) · GW(p)
I remember reading some speculation that Zinc supplements and (separate speculation) garlic supplements might have some beneficial effect against COVID19, but can't find the source. Anyone knows what's the status on that?
comment by Gunnar_Zarncke · 2020-03-15T21:15:18.279Z · LW(p) · GW(p)
I have seen quite a bit of advice here or elsewhere but not so much what people actually do. I'd like to post a poll but unfortunately that is no longer possible. But maybe you can comment here what you do.
In the spirit of this question I have written this on my FB page:
https://www.facebook.com/gunnar.zarncke/posts/1142992466050982
comment by Leon Lang (leon-lang) · 2020-03-15T16:48:59.208Z · LW(p) · GW(p)
Is there anything precise known about the distribution over the severity of symptoms I should expect as a 20-30 year old? I'm in that age-group, that's why I'm interested.
So, what I'd like to know specifically, conditional on being infected, is:
- How likely would I be asymptomatic?
- How likely would I have symptoms not more severe than the common cold?
- How likely would symptoms comparable in severity to the flu (being mostly in the bed for maybe 2 weeks but nothing more)?
- How likely would I have mild to moderate pneumonia with which I could still stay at home?
- How likely would I need to go into the hospital and receive oxygen, but no mechanical ventilation?
- How likely would I need mechanical ventilation?
- How likely is it I might die even if I receive mechanical ventilation?
comment by TurnTrout · 2020-03-15T02:28:29.403Z · LW(p) · GW(p)
My roommate tested positive for type A flu. Does this mean he is unlikely to have COVID?
Replies from: habryka4, James_Miller↑ comment by habryka (habryka4) · 2020-03-15T05:47:33.935Z · LW(p) · GW(p)
Comorbidity is low, from what I remember, so I do think a positive non-COVID case is pretty indicative and should revert your risk-estimate relatively close to population level (I think, probably a factor of two higher or so, would be my random guess).
Though I would strongly recommend continuing to measure fever and ideally use one of those oxygen-level measurement thingies that would allow you to notice if things get really bad and you should definitely go to a hospital.
↑ comment by James_Miller · 2020-03-16T16:51:07.750Z · LW(p) · GW(p)
Greg Cochran told me in one of our podcasts that having the flu probably provides protection against getting COVID19 because having the flu activates your immune system.
comment by ChristianKl · 2020-03-14T19:16:32.558Z · LW(p) · GW(p)
It's a mystery for me why https://www.lesswrong.com/posts/aqTwwvBv84rjqKvnk/why-isn-t-increasing-ventilation-of-public-spaces-part-of [LW · GW] hasn't received any votes. It seems to me a very crucial question which a lot of possible upside if we get it right and get the information out about a easy to implement beneficial intervention.
Replies from: Raemon↑ comment by Raemon · 2020-03-14T19:24:20.212Z · LW(p) · GW(p)
I think the answer is most likely "there's just tons of coronavirus content right now and it's hard for people to keep track of it all."
I'm hoping in the nearish future we can do some retrospective organizing of the existing questions and try to prioritize them.
comment by Liron · 2020-03-14T12:12:01.419Z · LW(p) · GW(p)
This seems like a good time to sign up you and your loved ones for cryonics
Replies from: DanielFilan↑ comment by DanielFilan · 2020-03-14T16:42:15.225Z · LW(p) · GW(p)
FWIW I suspect cryonics orgs may not have capacity to handle the increased case load over the next few months.
Replies from: TurnTrout, DanielFilan↑ comment by DanielFilan · 2020-03-14T16:42:53.998Z · LW(p) · GW(p)
Although I'd love to be proven wrong about this.
comment by Gunnar_Zarncke · 2020-03-09T20:14:52.910Z · LW(p) · GW(p)
This is an interesting timeline of people in different countries (or speaking different languages) looking for information on the corona virus - based on Wikipedia view stats:
https://towardsdatascience.com/coronavirus-interest-inwikipedia-by-language-1b3e6562040d
comment by streawkceur · 2020-03-30T12:25:48.717Z · LW(p) · GW(p)
EDIT: The South Korean press releases contain a chart somewhat like the one I wanted, see e.g. https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030
I am looking for a better overview of imported cases by country of origin in East Asian countries.
EDIT: I remembered incorrectly, the following is wrong. In particular, I recall a statistic according to which a significant number of imported cases in South Korea in one day ~1-2 weeks ago came from China (~12, vs ~40 Europeans).
If this is true, this would seem to me like strong evidence that China is lying about having all domestic cases isolated, and community spread suppressed.
comment by syllogism · 2020-03-28T13:07:35.441Z · LW(p) · GW(p)
Does COVID-19 have a long "incubation period" because we don't have any immunity to it?
This is a "makes sense to me" idea I merely thought of, and I have 0 medical expertise. So this is probably dumb, but now that I've thought of it I keep wondering whether it's true.
My thinking is that the early symptom onset we feel when we get a cold or flu is partly down to our immune system responding, which causes inflammation etc. With the novel coronavirus, the immune system isn't responding early on, and the infection itself will be in the slow ramp stage of its exponential growth, so the infection is already well established by the time you start to feel it.
comment by ignoranceprior · 2020-03-25T19:45:01.636Z · LW(p) · GW(p)
Does anyone have thoughts on the recent Oxford study that claims that only a very small minority of infections lead to hospitalization or death, and that >50% of the UK population is already infected?
https://www.dropbox.com/s/oxmu2rwsnhi9j9c/Draft-COVID-19-Model%20%2813%29.pdf
Replies from: Wei_Dai, None↑ comment by Wei Dai (Wei_Dai) · 2020-03-25T21:12:49.930Z · LW(p) · GW(p)
Does anyone have thoughts on the recent Oxford study that claims that only a very small minority of infections lead to hospitalization or death, and that >50% of the UK population is already infected?
https://twitter.com/CT_Bergstrom/status/1242611599405277184
Replies from: Nonecomment by leggi · 2020-03-24T16:00:33.940Z · LW(p) · GW(p)
I've just stumbled across this press report:
A man has died and his wife is under critical care after the couple, both in their 60s, ingested chloroquine phosphate, an additive commonly used at aquariums to clean fish tanks. Within thirty minutes of ingestion, the couple experienced immediate effects requiring admittance to a nearby Banner Health hospital.
No mention of how much they ingested.
Chloroquine phosphate for fish-tanks, not human grade.
But a little knowledge without understanding can be a dangerous thing ...
comment by zby · 2020-03-23T13:18:11.401Z · LW(p) · GW(p)
A meta question - can we find areas with mismatched incentives (à la https://equilibriabook.com/ ), and biases, where the applying the rational thinking methodology would have high leverage? What can LessWrong do better than official science?
Replies from: ChristianKl↑ comment by ChristianKl · 2020-03-23T18:13:21.532Z · LW(p) · GW(p)
I don't think that there's a single "rational thinking methodology". We have a bunch of different tools.
While the current FDA works at allow Moderna to do their human trials very early, it seems the same isn't true for the EMA and CureVac who advises CureVac to do their first human trial only in early summer. Getting the public to be angry at the EMA for giving advice that delays a potential vaccine might be a point of high leverage.
There seems to be a strong need to get the educated public informed about the vaccine development business, so that we can exert public pressure on making it faster at the right points.
https://www.lesswrong.com/posts/SQDKMFmJToYqhZT5d/mrna-vaccine-development-for-covid-19 [LW · GW]
https://www.covid-watch.org/ for not privacy violating smart phone contact tracing is high leverage that might not get enough support from existing institutions.
Quantified Self has many points where the existing institutions aren't yet focused enough.
https://www.lesswrong.com/posts/6kj6cbcsMQFt4ntd9/using-the-quantified-self-paradigma-for-covid-19 [LW · GW]
comment by zby · 2020-03-20T10:09:02.615Z · LW(p) · GW(p)
Favipiravir - I have not seen this yet here, but it looks actually even more promising than chloroquine: https://en.wikipedia.org/wiki/Favipiravir
Reduction from 11 to 4 median days of treatment.
comment by Lucent · 2020-03-17T15:38:45.709Z · LW(p) · GW(p)
As a child who repeatedly got tonsillitis several times a year, sometimes when totally isolated and sometimes later hearing everyone else around me also got a sore throat, I grew up confused as to why contagious disease tracking was a problem we'd given up on and accepted. No doctor was ever curious of the specific virus or bacteria which caused it. While no one case greatly affected my life, as a whole they very much did. Then again, I was also struck by the possibly false realization that many STDs which have followed us for thousands of years could be permanently wiped out by a couple weeks of global abstinence.
Might we begin to have an intersection of low cost, widely-available tests for every strain of most every contagious agent along with a belief that contagions running amok in civilization is not an unchangeable reality after all this? These at-home DNA tests will soon hit a critical mass of data to link together a global family tree of every human--a previously unthinkable reality that'll suddenly become possible. I'm ready for such a critical mass in contagion tracking that makes a light bulb go off in our collective heads that contagion no longer be an essential part of civilization. Feel slightly sick or have been around someone coughing? We mailed you an envelope of 6 paper swabs for the back of your tongue that'll change color when exposed to the viruses we're aware are circulating in your area.
Learning that a specific RSV strain overwhelmed a daycare and infected 6 babies because my cough I got on a trip to a hotel upstate was cleaned by a chambermaid who got it from... would strongly alter my belief about the inevitability of even minor contagions in the same way the person to person tracking and quarantining of Coronavirus cases is radically altering our social and hygiene landscape right now. Even if widespread testing only shook the "people just get sick for a couple weeks once or twice a year; it happens" attitude of inevitability, it'd be worth it for that alone once it was economically feasible.
comment by DirectedEvolution (AllAmericanBreakfast) · 2020-03-15T19:06:24.586Z · LW(p) · GW(p)
I'm gathering info on anti-COVID-19 drug efforts. Here is what I've compiled so far. I've combined the number of trials in various phases with big data on expected success rates for drugs in those phases to forecast an 80% probability that at least one drug currently in phase 1-3 testing will be approved. Because trial efforts are unusual, I've used the following categories in my model:
0: pre-trial (not factored into probability of success)
1: new drug in early testing
2: approved drug being tested against COVID-19
3: official phase 3 trial
This is just the product of a morning's research, so if anybody finds better information, I'd appreciate it if you'd link a source so I can include it.
Remdesivir is the drug we'll know about soonest - one expert is quoted as saying in a couple months, so around May 2020. Other analysts say they're optimistic that production can be scaled up quickly. It treats the pneumonia of severe cases, so it might cut down on mortality. Other treatments are also being tested.
The CDC projects that "In the coming months, most of the U.S. population will be exposed to this virus." If the virus grows exponentially, the relative timing of a Remdesivir rollout and a COVID-19 explosion could matter hugely in terms of mortality.
Remdesivir has been administered via compassionate use permission already for at least 15 patients who weren't part of the trial (which is recruiting volunteers now). So although we won't know its effectiveness for a while, if it is effective, it can potentially begin saving lives immediately via compassionate use permission.
comment by Liam Donovan (liam-donovan-1) · 2020-03-15T08:51:00.774Z · LW(p) · GW(p)
Is this the right kind of copper tape for keeping surfaces virus-free? I'm concerned because it doesn't seem to have sharp edges, which I've heard is a big issue with the right kind of tape
https://smile.amazon.co.uk/Selected-Repellent-Copper-Conductive-Adhesive/dp/B07TV26465/
Replies from: jimmy↑ comment by jimmy · 2020-03-18T20:26:05.947Z · LW(p) · GW(p)
Yes, that looks right. The edges of any thin tape are going to be sharp, it's just that copper is strong enough to hold that geometry instead of folding easily before it cuts you.
Replies from: liam-donovan-1↑ comment by Liam Donovan (liam-donovan-1) · 2020-03-19T20:23:04.835Z · LW(p) · GW(p)
Well that's why I was concerned that this tape doesn't have sharp edges!
Replies from: jimmycomment by willbradshaw · 2020-03-15T08:43:48.258Z · LW(p) · GW(p)
I'm working on a document / series of posts about coronavirus biology – viral structure, replication cycle, that sort of thing. This is mostly for my own education but I figure it's also a useful exercise to make the result public in a presentable form. I'm posting this here (a) as a commitment device to get something out in the next week or so, and (b) to see if anyone has any questions they'd like answered in this area that I could look into.
Currently I'm mainly learning about coronavirus biology in general, expect to switch to COVID19 specifically in a couple of days.
Replies from: sprague, zby↑ comment by sprague · 2020-03-15T16:48:55.436Z · LW(p) · GW(p)
check out: http://virological.org/uploads/short-url/z0cOhZzme3C6HtlcOcE61uMwJmU.pdf
Replies from: willbradshaw↑ comment by willbradshaw · 2020-03-15T22:19:28.285Z · LW(p) · GW(p)
Thanks but I'm not asking for sources. I have lots of sources already.
↑ comment by zby · 2020-03-15T10:51:10.982Z · LW(p) · GW(p)
The best article for an interested lay person I have seen is this The Economist article: https://www.economist.com/briefing/2020/03/12/understanding-sars-cov-2-and-the-drugs-that-might-lessen-its-power
Here is an outline: https://outline.com/Ma9nV7
Replies from: willbradshaw↑ comment by willbradshaw · 2020-03-15T11:41:56.039Z · LW(p) · GW(p)
Thanks, this is a nice layman's overview. I'm not a layman, though, and I'm planning on going much deeper than this (I've spent a lot of my weekend buried in virology textbooks).
From the article: "HIV and SARS-CoV-2 have about as much in common as a human and a satsuma" I wonder whether this is just journalistic flair or actually grounded in something. They don't cite their sources very well, unfortunately.
comment by benyeoh · 2020-03-14T20:01:54.763Z · LW(p) · GW(p)
Is COVID really helping the environment? Some articles suggest there's a postive short term impact from lower air pollution, but when I looked at long term CO2 in the atmosphere there's been no impact. Would be interested in thoughts? Blog here: https://www.thendobetter.com/investing/2020/3/12/no-impact-seen-on-atmospheric-co2-in-q1-2020
comment by KevinO · 2020-03-14T18:39:44.135Z · LW(p) · GW(p)
Edit: apparently the cited study does say that no viable SARS-COV-2 virus was found on the copper after 4 hours.
Original comment:
Dr. Peter Hotez said on the podcast The Drive (https://peterattiamd.com/peterhotez/) that a new (March 13) paper (https://www.medrxiv.org/content/10.1101/2020.03.09.20033217v2) found that SARS-COV-2 could last for 8-24 hours on copper. If you search for "copper" in the show notes you'll find the 8-24 hour figure.
comment by qirlib (kirill-belov) · 2020-03-14T05:17:37.035Z · LW(p) · GW(p)
Is it possible to quickly develop (within 24h) respiratory failure or breathing difficulties without having severe onset symptoms (i. e. fever, perhaps chest pain (chest congestion) or unstoppable cough)? Which symptoms exactly should be looked out for? If the possibility of suddenly going straight to blue is unavoidable, what is the distribution of how exactly physically able and mentally coherent you are likely to become when that happens?
(personalized: There's a considerable probability I'm already infected and my isolated space is located in a rather obscure place which is about 1.5km from the nearest road where ambulance can adequately reach me. I need a clear-cut line for when I should orderly organize for me to be transported back to civilization. If this line is not reliable or something goes very wrong, how likely it is that I would be able to walk 1.5km in emergency condition, with -10 Celsius outside, all by myself?)
Replies from: pktechgirl↑ comment by Elizabeth (pktechgirl) · 2020-03-14T05:28:47.897Z · LW(p) · GW(p)
According to https://www.facebook.com/jeanqasaur/posts/10111638281986401 , symptoms are often not sudden onset, but my impression is it can get worse quite suddenly, as the virus moves from upper to lower respiratory system. The primary way to know if things are getting serious is shortness of breath, but, uh, that seems really bad to wait for if you need to walk a mile to get help.
This is really speculative on my part, but: this might be a good candidate for a pulse/ox meter. Normally I think they aren't very useful because you can go by symptoms, but it might (might) be useful in your case, if you can monitor frequently enough to catch a dropping oxygen concentration before it interferes with your breathing (I do not know if the meters are accurate enough to do this).
Replies from: ErickBall↑ comment by ErickBall · 2020-03-14T22:00:19.021Z · LW(p) · GW(p)
Hopefully someone more knowledgeable can weigh in, but in the meantime I want to sound a note of caution on this: my experience with pulse oximeters is that by the time it drops noticeably below normal, you are already quite sick and walking a mile may not be practical. The point of the pulse ox is more to be able to quantify your symptoms so that you can have a specific threshold for when you should seek emergency treatment. I don't believe it's a leading indicator and so it may not be helpful for this situation.
comment by jmh · 2020-03-12T12:32:43.599Z · LW(p) · GW(p)
Drive through screening test? Would they be good for the USA and EU?
comment by jmh · 2020-03-12T12:12:36.098Z · LW(p) · GW(p)
Just looked at a link for a Vox article that popped up when I launched my browser. Nice chart but would be interesting to know some thing about the model parameters (and I think the graph is illustrative not anything factual or based on some model CDC has) that would be required to achieve the image, and some sense about how close both USA and EU are to achieving the parameter values.
I thought the interesting thing about is was that the goal is not really about reducing the number of infections. That is not really a narrative that is in the public media at this time -- or I'm missing it.
Replies from: AlexSchell↑ comment by AlexSchell · 2020-03-12T18:27:26.202Z · LW(p) · GW(p)
I made a model that tries to replicate the chart, see here [LW(p) · GW(p)].
Replies from: jmh↑ comment by jmh · 2020-03-12T20:52:23.329Z · LW(p) · GW(p)
Thanks. BTW, have you thought about putting an average recovery/dies period in, perhaps differing based on hospital bed or ICU and look at how those parameters might shift things a bit? Might even be good to model the time between infection and need for medical care (be that bed or ICU).
Or are those implicit in your beta and gamma values?
comment by Josh Jacobson (joshjacobson) · 2020-03-11T23:01:17.791Z · LW(p) · GW(p)
Take someone in the U.S. who is heavily immunocompromised, such that their risk of death from any infection beyond a mild cold averages to 15%, and assume that their risk of death from coronavirus is 100%. Assume they've been employing social distancing tactics as a result for some time.
Is there available information or projections on whether the total risk for this person has increased or decreased as a result of coronavirus?
A key assumption/the reason it may have decreased is that we could expect that the prevalence of all other diseases is falling due to the social distancing tactics being employed for coronavirus.
comment by vidro3 · 2020-03-10T12:07:48.447Z · LW(p) · GW(p)
1) are we going to create some super-bacteria by using a ton of hand sanitizer and wipes?
2) Is this report of 40-70% infection rate world-wide reputable, realistic, useful?
In my view we don't know what percentage of infections result in a) symptoms, b) serious symptoms. It's pretty easy to take those estimates coupled with current death rates and get a result of 100million deaths due to COVID-19. That seems super extreme and unlikely to me.
I'm not sure the usefulness of stating a 40-70% infection rate if the rate of critical symptoms within that group is only ~10%
Replies from: TobyBartels↑ comment by TobyBartels · 2020-03-15T18:27:55.557Z · LW(p) · GW(p)
- Alcohol and bleach are both extremely common in our current environment, so if it's possible to create these superbugs, then we should already be doing it, although this could speed up the process. And quick Google searches tell me that nothing is evolving resistance to bleach; but we are indeed creating alcohol-resistant superbugs that are starting to infest hospitals. So those may get worse.
comment by Thomas · 2020-03-27T15:33:46.488Z · LW(p) · GW(p)
CROSSPOST from my blog:
https://protokol2020.wordpress.com/2020/03/27/covid-19-a-view-to-a-kill
The R0 factor for this illness, which denotes the average number of people infected by a carrier, isn't a constant, it's a function of time. R0 = R0 (time). In fact, it's a function of more parameters and not just time. For example, if quarantined, R0 should be close to 0. There are many unknown factors here, of course, some even known. Some push this now well known R0 term bellow 1, others above 1. It's all about reducing R0 below 1, and the illness will die out. Otherwise, the number of sick people will go through the roof, by the exponential growth function manner.
All of the above is very well known and understood and repeated over and over again now.
Then you get infected, you caught the virus somehow, what now? Your cells will spread the virus among each other by the factor R0IC !
R0IC is the average number of cells, one infected cell will further infect on average. "IC" in standing for "Inter-Cellular". This is again not a constant but is a function of time and many other known and unknown factors. For example time, temperature, the immune system activity and so on. R0IC = R0IC (t, T, ISactivity, ..., ). At least as complex as the transmission factor R0 between humans, is the transmission factor R0IC between cells. When R0 falls bellow 1 for a considerable time period, the epidemics burn out. When R0IC falls bellow 1 for a considerable time period, the particular human's illness burns out.
The last paragraph above is a less well-known fact, but it's a fact none the less. Spreading of this virus among cells, in a way closely imitates the spreading among humans. Medical doctors and medical nurses work hard to minimize R0IC in already infected people. They might call it differently, but it is what it is. Stoping the intercellular infection, "flattening the curve" inside the patient's body, "delaying the disease" inside the patient's lungs -- you name it! Medical professionals thus "delay the disease" inside you, hoping that the immune system will kick in and do the same until done.
Now, when you are infected and breath, you inhale more or less clean air and exhale quite a lot of viruses. Soon, you are inhaling some previously exhaled viruses back and some of those might infect an additional lung cell. By breathing through SCUBA, there are no previously exhaled viruses and therefore this R0IC should go down slightly, shouldn't it? By breathing some higher oxygen concentrations than normal, this R0IC should go down even more. Since oxygen is a bit toxic for COVID-19.
By breathing some WARMER air than normal, this R0IC should go down even more, since the COVID-19 virus doesn't like hot air, does it? Especially if the air is salty or smells of some detergent, pure alcohol and so on, it's killing the viruses. Some even inside your nose and downward, perhaps.
Then, you may, sometimes after infection, during the asymptomatic phase, run up the hill in sunny weather. Puffing like an old locomotive, you will exhale a lot of viruses. Fortunately, nobody is with you and those exhaled viruses will die under the Sun. Again, you even so slightly decreased the R0IC factor and "flattened the curve" of the internal infection between your cells. You may as well try to inhale some eucalyptus hot vapors under the towel, as they suggest already. Perhaps you should insulate yourself in a sauna. Not too hot, not too humid, but just enough for you to survive and not the virus. Under medical control, of course!
And then perhaps, medical doctors should think about their doctrinal procedures for COVID-19 in this light and to refine these suggestions above considerably. I am no medical doctor! But then again, Marylin Vos Savant was no mathematician either but gave a valuable lesson to Paul Erdos himself. There are times when IQ matters the most.
Anyway. When and if you are infected with COVID-19, in the presymptomatic phase, keep the R0IC down as much as you possibly can. The second symptomatic phase may never come. Doing so, you will (ever so slightly) lower the R0 too!